
Abstract
The present study sought to examine the occurrence and correlates of depression, PTSD, and insomnia in a cohort of Palestinian refugees residing in camps located in Jordan during the outbreak of the War on Gaza on Oct.7th.This is a cross-sectional cohort study that employed the convenient sampling method to recruit Palestinian refugees residing in Irbid and Azmi Almufti camps for Palestinian refugees. Depressive symptoms were assessed using the Patient Health Questionnaire (PHQ-9) scale. The self-reported PTSD symptoms were evaluated using the brief PTSD scale, and insomnia severity was assessed using the Insomnia Severity Index -Arabic scale (ISI-A). The data analysis from 258 participants showed that severe depression was reported in 178 participants (69%). Additionally, 127 participants (49.2%) reported severe PTSD symptoms, and 156 participants (60.5%) reported severe insomnia symptoms. Regression analysis revealed that “Residents of Azmi Almufti camp” was a significant correlate for severe depression (OR = 2.22, 95% 1.28–3.85, p = 0.004) and severe PTSD (OR = 1.81, 95% CI = 1.10–2.99, p = 0.02). The use of over-the-counter antihistamines as a sleep aid was a significant correlate severe insomnia (OR = 3.19, 95%CI = 1.17–8.71, p = 0.02) and PTSD (OR = 3.32, 95% CI = 1.34–8.21, p = 0.01). The conflict in Gaza has been observed to correlate with mental health challenges, particularly among Palestinian refugees residing in Jordan.
Similar content being viewed by others

Explore related subjects
Discover the latest articles and news from researchers in related subjects, suggested using machine learning.Avoid common mistakes on your manuscript.
1 Introduction
The existence of Palestinian refugees in Jordan is mainly linked to two major dates: 1948 and 1967. In 1948, a war erupted between Israel and the Arabs, resulting in the occupation of almost 77% of Palestinian land by Israel. This catastrophe is known in the Arab world as the Nakba. In 1967, another war erupted between Israel and the Arabs known as Al Naksa, ending with the occupation of new territories including, the Gaza Strip, Sinai Peninsula, the West Bank, and the Golan Heights. Besides the suffering and oppression of Palestinians that resulted from the two defeats, hundreds of thousands were forced to flee their homeland for neighboring countries such as, Lebanon, Syria and Jordan. The number of Palestinian refugee camps in Jordan is 10 official camps recognized by UNRWA (United Nations Relief and Works Agency), and 3 unofficial camps, namely the Prince Hassan Camp, the Madaba Camp, and the Sahab Camp. Palestinians residing in refugee camps are fragile economically and health wise, specifically those who reside in Azmi AlMofti Refugee Camp in Irbid. Moreover, The 35,000 Palestinian refugees residing in Azmi AlMofti Refugee Camp are confronting challenging conditions related to housing, education, humanitarian assistance, healthcare, and social welfare [1,2,3].
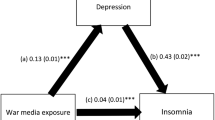
Mental health distress is known to be triggered or exacerbated by continuous exposure to horrific war scenes such as killing civilians, including women and children and bombarding houses, and hospitals [4]. The adverse impact on mental health stemming from exposure to certain content on social media and other communication resources primarily manifests as depression, post-traumatic stress disorder (PTSD), and insomnia. [5, 6].
Although continuous studies are highlighting the mental health challenges faced by Palestinians living in their homeland under occupation [7, 8], less evidence has examined the mental health status of the Palestinians residing in refugee camps in Jordan. According to the estimates, about 370,000 Palestinians live in refugee camps distributed in various Jordanian districts. This population is highly vulnerable to mental health distress due to the ongoing armed conflict in Palestine, their homeland, poverty, unemployment, and the challenging environment in their camps [9].
Therefore, the present study sought to examine the occurrence and correlates of depression, PTSD, and insomnia in a cohort of Palestinian refugees residing in camps located in Jordan, namely Irbid and Azmi Almufti camp located in Irbid, 80 km north of Amman, the capital, during the outbreak of the War on Gaza on October 7th.
2 Material and methods
2.1 Study design and settings
This is a cross-sectional cohort study that employed the convenient sampling method to recruit Palestinian refugees residing in Irbid and Azmi Almufti camps.
The study participants were enlisted through on-site visits. All procedures adhered to the principles outlined in the Declaration of Helsinki, and the research protocol was approved by XXXX University IRB committee. Informed consents were obtained from all participants. The research team communicated the study's objectives to potential participants through in-person interviews. Those who chose to participate were invited to sign a consent form; they retained the autonomy to discontinue their involvement at any stage. Data collection occurred in January 2024. A statistical G power calculation for logistic regression determined that a minimum of 250 participants were necessary for the study.
2.2 Study instrument
The study instrument consisted of the covariates part and the outcome variable part. The covariate part comprised demographics and social media interaction concerning the war on Gaza. The outcome variables assessed were PTSD, depression, and insomnia symptoms.
2.3 Covariates
This section crafted structured inquiries aimed at gathering demographic information from participants. Specifically, participants were asked to provide details regarding their age, gender, marital status, employment status, highest level of education attained, smoking habits, presence of chronic illnesses, and use of chronic medications. Participants were asked whether they have relatives or friends residing in Gaza and how they overcome their sleeping problem by using over-the-counter (OTC) sedating antihistamines as sleep aids or household homeopathic relaxing remedies. Additionally, participants were asked about the frequency with which they share news related to the Gaza war and their opinions on temporarily abstaining from social media interactions to mitigate potential mental health impacts.
2.4 Outcome variables
2.4.1 Depression symptoms
The self-reported depressive symptoms were assessed through the Patient Health Quality-9 scale (PHQ-9) Arabic version. This validated scale provides a comprehensive capture of depression symptoms through nine questions rated against Likert-type answers. A score above 14 indicates severe depression. [10, 11]
2.4.2 Post-traumatic stress disorder symptoms
The self-reported PTSD symptoms were evaluated using the brief PTSD scale originally developed by Foa et al. 1993, translated to Arabic, and validated by [12] with a Cronbach alpha of 0.79. The scale consists of 17 questions to capture PTSD symptoms according to the DSM-IV guidelines. A score above 25 on this scale reflects severe PTSD symptoms.
2.4.3 Insomnia symptoms
The assessment of the self-reported insomnia burden was conducted through the Insomnia Severity Index Arabic version (ISI-A). This validated and reliable scale (Cronbach alpha = 0.81) comprises 7 questions that explore sleep quality for the past week, with a total score range between 0 and 28. A score exceeding 14 indicates severe insomnia. [13, 14]
2.5 Data analysis
Data were analyzed using SPSS software version 21. The demographic information of the participants was expressed as frequencies and percentages. Three outcome variables (dependent variables) were found in the study: depression, PTSD, and insomnia. Therefore, three distinct binary regression analyses were carried out. Initially, to identify the potential confounders, a univariate analysis was performed to identify the potential confounders showing p < 0.1, which were used to feed the multivariable binary regression model using the backward stepwise approach to identify which factors are independently associated with each of the outcome variables. A p-value of less than 0.05 was considered to be statistically significant.
3 Results
3.1 Participants characteristics
The data analysis from 258 participants showed that 166 (64.3%) were males, 173 (67%) were aged above 26 years, 137(53%) were married, 133 (51.5%) were residents of Irbid camp, 160 (62.01%) were employed, 83 (31.9%) reported having relatives or friends in Gaza, 45 (17.44%) reported losing a family member or a friend in Gaza, 29 (11.2%) reported using self-medication with OTC sedating antihistamine to improve sleep, and 16 (6.2%) reported using self-medication with herbal homeopathy to improve sleep. Table 1.
3.2 Depression: occurrence and correlates
The severity of depression was assessed through the PHQ-9 scale Arabic version, participants scoring 15 and above were considered severely depressed. Therefore, our analysis revealed that 178 participants (69%) reported severe depression. To identify the factors that could be potentially associated with severe depression, a univariate analysis was conducted. The potential confounders: “age”, “marital status”, resident of Azmi Almufti camp”, “employment”, “using OTC antihistamines as a sleep aid”; and long-term medications were identified and used to feed the subsequent multivariable model, which was performed using the backward stepwise model. The multivariable model finally included “resident of Azmi Almufti camp” as a significant correlate for severe depression (OR = 2.22, 95% 1.28–3.85, p = 0.004). Table 2
3.3 PTSD: occurrence and correlates
We used the Arabic-validated Scale [12] for assessing the self-reported PTSD symptoms with a cut-off score above 25 for severe PTSD symptoms. We report that 127 participants (49.2%) reported severe PTSD symptoms. The univariate analysis was carried out to identify the potential confounders of severe PTSD. We report that “smoking”, “Resident of Azmi Almufti camp”, “posting the war news on social media”, and “using OTC antihistamines as a sleep aid” were regarded as potential confounders and were further used to build the multivariable binary logistic regression model as above. The multivariable model finally included “Resident of Azmi Almufti camp”, and “using OTC antihistamines as a sleep aid” as significant correlate for severe PTSD (OR = 1.81, 95% CI = 1.10–2.99, p = 0.02) and (OR = 3.32, 95% CI = 1.34–8.21, p = 0.01) respectively. Table 3.
3.4 Insomnia: occurrence and correlates
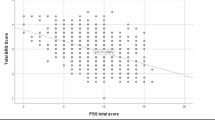
Insomnia was assessed using the ISI-A scale, with a threshold score above 14 used to screen for severe insomnia symptoms. A total of 156 participants (60.5%) reported severe insomnia symptoms. The univariate analysis identified “receiving long-term medications for chronic diseases” and “using OTC antihistamines as a sleep aid” as potential confounders. The multivariable binary logistic regression showed that only using OTC antihistamines as a sleep aid” was a correlate for severe insomnia (OR = 3.19, 95%CI = 1.17–8.71, p = 0.02). Table 4.
4 Discussion
The present study aimed to identify the occurrence and correlates of depression, PTSD, and insomnia as self-reported symptoms in a cohort of Palestinian refugees residing in Jordan during the outbreak of the War on Gaza. We report a high rate of all the above-mentioned symptoms. Also, our findings revealed that the residents of Azmi Almufti camp were at higher risk for severe depression and PTSD symptoms. In addition, using sedating antihistamines as a sleep aid was associated with severe PTSD and insomnia symptoms.
This huge burden of depression and PTSD in the study sample is attributed to multifactorial, interrelated, and complicated factors, a nexus worth exploring. Our findings demonstrated that the refugees residing in Azmi Almufti camp were more prone to severe depression and PTSD. Exploring mental health status in this population is faced with social and cultural barriers [9]. Poor living conditions, poverty, and a lack of jobs could explain, at least in part, this finding. According to published data dated back in 2011, Azmi Almufti camp is the second poorest camp with the highest rate of unemployability in general and in women reaching up to 18% in total and 25% for females [15]. Although no updates are yet available about the socio-economic status of the Azmi Almufti camp, however, the authors expect a more challenging situation due to the Syrian conflict that has led to Syrian refugees migration mainly to Irbid, thus posing additional restrains on Jordan, the hosting country.
Poor mental health status encompasses the behavior of individuals to adopt negative behaviors, for example, in a cross-sectional study comprising more than 73,000 Palestinians living in Jordan camps, depressive symptoms were associated with days of missing schools, the same study points out the high rates of depressive symptoms namely loneliness, suicidal ideation, and worry among adolescents [16].
The findings of this study highlighted that participants using OTC sedating antihistamines as a sleep aid were at higher association for severe insomnia and PTSD symptoms. Self-medication with sedating antihistamines is a common practice in many populations due to its availability, safety, and affordability [17]. In addition, earlier, our research group demonstrated that OTC sedating antihistamines are the most recommended sleep aid by community pharmacists in Jordan [18]. Our findings can be explained as follows: participants experiencing severe insomnia and PTSD symptoms tend to use the “available” medications to alleviate their symptoms, conversely, these severe symptoms could be due to antihistamines, as they stimulate the Central Nervous System, which could result in difficulty sleeping or insomnia or users may take overdoses of antihistamines due to tolerance [19]. According to the literature, the clear benefits of sedating antihistamines have not been proven yet [20, 21]. Similarly, antihistamines are ineffective in alleviating PTSD symptoms. Furthermore, they could exacerbate symptoms due to their complex pharmacological actions [22]. This is the first study, to the best our knowledge, that highlighted the occurrence and correlates of depression, PTSD, and insomnia experienced by the Palestinian refugees residing in Jordan during the outbreak of the October7th war in their homeland in Palestine- Gaza. Although the current study has several strengths, including the unique sample type, the validated scales, and the sound data analysis performed, some limitations exist. For example, the study did not include a follow-up phase to monitor the changes in the mental health spectrum of the participants, also, the study did not provide a thorough psychiatric assessment by specialists in the camps due to social and cultural barriers to mental health.
5 Conclusion
In conclusion, the impact of the ongoing war on Gaza demonstrated to be associated with mental health distress outside the borders of Gaza. Palestinian refugees residing in Jordan for decades are highly affected mentally. Comprehensive and immediate actions are warranted to address the mental health and well-being of this vulnerable community by addressing the modifiable correlating factors.
Data availability
The data will be provided by the corresponding author upon request.
References
Bocco R. UNRWA and the Palestinian refugees: a history within history. Refug Surv Q. 2009;28:229–52.
Akram S. UNRWA and Palestinian refugees. Oxford Handb Refug forced Migr Stud. 2014;
Irfan AE. Educating Palestinian refugees: the origins of UNRWA’s unique schooling system. J Refug Stud. 2021;34:1037–59.
Greinacher A, Derezza-Greeven C, Herzog W, Nikendei C. Secondary traumatization in first responders: a systematic review. Eur J Psychotraumatol. 2019;10:1562840.
Wiederhold BK. A legacy of trauma: how local conflicts can have global implications for mental health. Cyberpsychology, Behav. Soc. Netw. Mary Ann Liebert, Inc., publishers 140 Huguenot Street, 3rd Floor New; 2023. p. 803–4.
Mahamid FA, Berte DZ. Portrayals of violence and at-risk populations: symptoms of trauma in adolescents with high utilization of social media. Int J Ment Health Addict. 2020;18:980–92.
Haj-Yahia MM, Greenbaum CW, Lahoud-Shoufany L. Palestinian adolescents’ prolonged exposure to political violence, self- esteem, and post-traumatic stress symptoms. J Interpers Violence. 2021;36:4137–64.
Giacaman R, Rabaia Y, Nguyen-Gillham V, Batniji R, Punamäki R-L, Summerfield D. Mental health, social distress and political oppression: the case of the occupied Palestinian territory. Glob Public Health. 2011;6:547–59.
McKell C, Hankir A. Barriers to treatment of mental health problems for Palestinian people in refugee camps in Jordan: a cross-sectional study. Lancet. 2018;391:S8. https://doi.org/10.1016/S0140-6736(18)30333-7.
AlHadi AN, AlAteeq DA, Al-Sharif E, Bawazeer HM, Alanazi H, AlShomrani AT, et al. An arabic translation, reliability, and validation of Patient Health Questionnaire in a Saudi sample. Ann Gen Psychiatry. 2017;16:1–9.
Kroenke K, Spitzer RL, Williams JBW. The PHQ-9. 46202:606–13.
Wadaa NN. Secondary traumatic stress symptoms in military parents of Iraqi army. Mustansiriyah J Arts. 2016;39.
Morin C. Insomnia: Psychological assessment and management. [Internet]. 1993. https://psycnet.apa.org/record/1993-98362-000. Accessed 2 Nov 2019.
Suleiman KH, Yates BC. Translating the insomnia severity index into Arabic. J Nurs Scholarsh. 2011;43:49–53.
Zhang ÅAT and H. The socio-economic conditions of Jordan’ s Palestinian camp refugees. 2011.
Nathani K, Lee WC, Taha S, Horino M, Seita A, Serag H. The Association Between Mental Well-Being and School Attendance Among Palestinian Adolescent Refugees in UNRWA Schools. J Child Adolesc Trauma. 2023;16:339–50. https://doi.org/10.1007/s40653-022-00460-7.
Farzam K, Sabir S, O’Rourke MC. Antihistamines. 2019;
Gammoh OS, Al-Smadi A, Turjman C, Mukattash T, Kdour M. Valerian: an underestimated anxiolytic in the community pharmacy? J Herb Med. 2016;6:193–7. https://doi.org/10.1016/j.hermed.2016.09.001.
Richardson GS, Roehrs TA, Rosenthal L, Koshorek G, Roth T. Tolerance to daytime sedative effects of H1 antihistamines. J Clin Psychopharmacol. 2002;22:511–5.
Culpepper L, Wingertzahn MA. Over-the-counter agents for the treatment of occasional disturbed sleep or transient insomnia: a systematic review of efficacy and safety. Prim care companion CNS Disord. 2015;17:26162.
Vande Griend JP, Anderson SL. Histamine-1 receptor antagonism for treatment of insomnia. J Am Pharm Assoc. 2012;52:e210–9. https://doi.org/10.1331/JAPhA.2012.12051.
Shiromani PJ, Keane TM, Ledoux J. Post-traumatic stress disorder: Basic science and clinical practice. Post-Traumatic Stress Disord Basic Sci Clin Pract. 2009;1–409.
Acknowledgements
The first author would like to thank Sama, Suzi, Yasmina, and Nour.
Author information
Authors and Affiliations
Contributions
(1) made substantial contributions to the conception (Omar Gammoh, Saleh Bazi) or design of the work (Omar Gammoh, Mervat Alsous); or the acquisition, analysis (Saleh Bazi, Ruba Al Akash), or interpretation of data (Bilal Sayaheen, Albara Alomari and Mervat Alsous); (2) drafted the work or revised it critically for important intellectual content (Omar Gammoh, Bilal Sayaheen, and Mervat Alsous); (3) approved the version to be published Omar Gammoh, Albara Alomari, Saleh Bazi, Ruba Al Akash, Bilal Sayaheen, and Mervat Alsous; (4) agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved (Omar Gammoh).
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The protocol was approved by Yarmouk University IRB committee in accordance with the Declaration of Helsinki. Informed consents (Consent to Participate) were obtained from all participants.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Gammoh, O., Bazi, S., Al Akash, R. et al. Assessment of depression, PTSD, and insomnia symptoms in a cohort of Palestinian migrants residing in Jordanian camps during the outbreak of the War on Gaza: occurrence and correlates. Discov Ment Health 5, 8 (2025). https://doi.org/10.1007/s44192-024-00124-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s44192-024-00124-y