
Abstract
Ovarian cancer (OC) is the fourth leading cancer form in Jazan, Saudi Arabia. However, limited awareness and delayed healthcare-seeking behaviors might negatively impact screening uptake and early diagnosis. This study aimed to assess awareness and knowledge of OC, and related risk factors among the female population of Jazan region, Saudi Arabia. A cross-sectional web-based survey was conducted asking questions about the general awareness, knowledge, and awareness of risk factors associated with OC using a self-administered questionnaire. Descriptive statistics, chi-square tests, and Pearson’s correlation analysis were used to analyze the data and a p ≤ 0.05 was considered statistically significant. Of the 465 participants, 433 completed the questionnaire (response rate = 93%). Internal reliability of questionnaire sections was found acceptable (Cronbach’s alpha = 0.794, 0.738, and 0.816). Alarmingly, a significant majority of respondents exhibited poor general awareness (85%), poor knowledge (89.1%), and poor awareness of risk factors (86.1%). Only a small tested population showed good to moderate awareness (14.9%), knowledge (10.9%), and awareness of risk factors (13.8%). Significant positive correlations were observed between OC awareness and knowledge (r = 0.60, p < 0.01), OC awareness and risk factor awareness (r = 0.515, p < 0.01), as well as between knowledge and risk factor awareness (r = 0.634, p < 0.01). Limited awareness of OC and its risk factors were noted in the women population of Jazan region which highlights the importance and critical need for targeted educational initiatives aimed to improve the general public understanding and to promote preventive and screening measures.
Similar content being viewed by others

Explore related subjects
Discover the latest articles and news from researchers in related subjects, suggested using machine learning.Avoid common mistakes on your manuscript.
1 Introduction
Ovarian cancer (OC) ranks the eighth most prevalent form of cancer among women worldwide and is a leading cause of gynecological cancer mortality. The total number of new OC cases in the year 2020 was reported to be more than 0.3 million worldwide (Torre et al. 2018; Ovarian Cancer Statistics 2020). Over 313,959 new cases and 207,252 deaths were reported globally in this year, with an age-standardized incidence rate (ASR) of 6.6 per 100,000 and a mortality rate of 4.2 per 100,000 (Huang et al. 2022). In Saudi Arabia, OC was responsible for 444 new cases and 281 deaths in the year 2020, accounting for 1.6% of all cancer cases, with an ASR of 3.8 per 100,000 a mortality rate of 2.7 per 100,000 (Global Cancer Observatory n.d.; Aga et al. 2022).
The insidious nature of the disease, characterized by peritoneal dissemination and limited early symptoms, contributes to its poor prognosis with a cure rate of merely 30% (Lengyel 2010). Therefore, early detection of OC is particularly crucial to achieve improved outcomes, yet public awareness remains inadequate. Early diagnosis of OC enables better treatment options which can significantly improve long-term survival rates, and enhance the quality-of-life (QoL) (Russo et al. 2009; Ottevanger 2017). Increasing awareness about the symptoms of OC and associated risk factors is one of the most effective strategies that can be adopted to reduce mortality by facilitating early diagnosis (Russo et al. 2009). Women over the age of 50, as well as those with a family history of OC, are at a higher risk of developing the disease (Alhedyani et al. 2016).
Previous research suggested that increased awareness of OC symptoms among women could increase their participation in the screening programs and encourage timely medical assistance (Aga et al. 2022; Russo et al. 2009; Keng et al. 2015). Preventative healthcare services provided by the obstetricians play a crucial role in reducing the risk of OC owing to their responsibility for educating and informing patients. As the number of OC cases in Saudi Arabia is increasing, it calls for an urgent need for studies that assess the women’s understanding of the warning signs and risk factors of OC (Aga et al. 2022; Alghamdi et al. 2014). On September, 12, 2020, the first virtual Saudi Women’s Cancer Summit was held by the Saudi Society for Internal Medicine (SSIM) at King Abdulaziz University and the Saudi Oncology Society (SOS), in collaboration with AstraZeneca, that brought along 441 specialists of women’s cancer (First Saudi Women’s Cancer Summit n.d.). Despite such initiatives, only a few studies have assessed OC knowledge and awareness among women in Saudi Arabia (Aga et al. 2022; Alhedyani et al. 2016; Alghamdi et al. 2014), and this study represents the first such effort in Jazan region of Saudi Arabia.
This study was aimed to evaluate the level of knowledge, awareness, and understanding of OC symptoms and risk factors among women in the Jazan region, which is located in the South-West of Saudi Arabia. Determination of the relationship between OC knowledge and socio-demographic and health factors was the second objective of this study. This study also explores the women perspective on OC risk factors and screening programs. Finally, it aimed to identify preventative and curative strategies to combat OC in the community.
2 Methods
2.1 Study background and participants
A cross-sectional observational survey included 465 female students of Jazan University and women from the general population of the region. The study was conducted between December 1, 2022, and October 31, 2023. Data collection was facilitated through a self-administered survey created using Google Forms, ensuring respondent anonymity. The survey link was disseminated through hospitals, healthcare facilities, and social media platforms such as Twitter and WhatsApp to reach female individuals aged 18 and above residing in the Jazan region. Snowball convenience sampling was employed to recruit participants through social media channels (Silva et al. 2022; Assiry et al. 2022; Ahsan et al. 2021). The target participants included general female population such as homemakers, students, and community women, who were prior instructed to select only response per question. The survey questionnaire was available in both Arabic and English languages.
2.2 Inclusion and exclusion criteria
Women from Jazan including the female students of Jazan University, who were aged between 18 to 60 years, were parts of the target population. The inclusion criteria specified participants who: (a) were women from the Jazan region aged 18 years and above, (b) provided informed consent, and (c) possessed sufficient comprehension of Arabic and/or English language. The exclusion criteria included: (a) women with a history of OC, and (b) individuals unable to provide informed consent.
2.3 Data collection tools
Data were collected using a self-administered, 30-items questionnaire which consisted of four sections. The first section comprised of seven questions asking the socio-demographic information and the medical history of the participants. The second section included five questions assessing awareness of participants about the OC. The third section consisted of ten questions aiming to assess the knowledge of participants about the OC, while the fourth section included eight questions exploring the awareness of participants about the OC risk factors.
2.4 Survey instrument development, validation, translation, and pilot study
The initial draft of the survey instrument was developed after meticulous, detailed, and extensive review of the relevant literature and careful deliberation by the authors (Huang et al. 2022; Aga et al. 2022; Lengyel 2010; Russo et al. 2009; Ottevanger 2017; Alhedyani et al. 2016; Keng et al. 2015; Alghamdi et al. 2014; Elshami et al. 2022). The prepared draft was reviewed for face and content validity by an independent expert committee comprising of one physician and two clinical pharmacists. Questions deemed inappropriate by the committee were eliminated, resulting into a finalized questionnaire with 30 items distributed across the four sections including Demographics, Awareness of OC, Knowledge about OC, and Awareness of OC risk factors.
To ensure linguistic appropriateness, the final English language version was translated into the Arabic version using forward–backward translation (Ahsan et al. 2021; Beaton et al. 2000; Degroot et al. 1994). A translator with expertise in both Arabic and English languages performed the forward translation, that was reviewed further by a bilingual author. Discrepancies were resolved in collaboration with the translator, if required. The final Arabic version questionnaire was back-translated into English by another author who had not seen the original English language version. Eventually, both versions were reviewed by all bilingual authors to ensure accuracy and consistency (Ahsan et al. 2021; Degroot et al. 1994).
The finalized questionnaire was piloted with an independent group of 30 participants to evaluate the usability and clarity of the questions (Browne 1995; Meraya et al. 2022). The pilot study revealed that the participants found the questions easy to understand and it took an average time of 10 min to complete the questionnaire. The validity and reliability of the developed survey instrument was confirmed during the pilot study. Face and content validity were assessed, and Cronbach's alpha was calculated to check reliability of the questionnaire. The samples from the pilot study were later excluded from the final analysis.
2.5 Reliability study
Cronbach's alpha was used to evaluate the internal consistency of individual items in each section of the study instrument. The alpha coefficients for all items exceeded the acceptable threshold of 0.70, confirming good reliability of the constructed scale (Fauville et al. 2021; Tavakol and Dennick 2011; Cronbach 1951). The specific alpha coefficients found for various sections of the study questionnaire were: Awareness of OC = 0.794, Knowledge about OC = 0.738, and Awareness of OC risk factors = 0.816.
2.6 Measures
2.6.1 Socio-demographic information
Participants were asked to provide information about their age group, exact age, gender, ethnicity (Saudi or non-Saudi), place of residence, education level, marital status, occupation, and medical history of both communicable and non-communicable diseases.
2.6.2 General awareness score of OC
The second component included five multiple-choice questions designed to assess the general awareness of respondents about OC. Respondents were asked to choose one of the following three options: ‘Yes’, ‘No’, or ‘I don’t know’. For instance, a sample question was “Are you aware of the importance of educating yourself about ovarian cancer through reading texts or watching related videos?” Each answer in ‘Yes’ was awarded one point, while responses ‘No’ and ‘I don't know’ received zero points (Assiry et al. 2022). The total awareness score was determined by summing up the points from all questions in the section. Higher scores indicated better overall awareness of OC among the tested population.
2.6.3 Knowledge score about OC
The third section consisted of ten closed-ended questions designed to evaluate the knowledge of participants about OC. Similar to the awareness section, respondents selected from the three options: ‘Yes’, ‘No’, or ‘I don't know’. An example question and an actual item on the list was: “Are most early-stage ovarian cancer patients symptomatic?". Each correct response earned one point, while incorrect or ‘I don't know’ responses received zero points (Assiry et al. 2022). The knowledge score was then calculated by aggregating the points for all questions of the section and higher scores reflected a stronger understanding of OC.
2.6.4 Risk factors awareness score about ovarian cancer
The fourth section of the questionnaire consisted of eight closed-ended questions aimed at assessing the awareness of respondents about the OC risk factors. Similar to previous questions, the awareness was assessed by choosing between the three options, ‘Yes’, ‘No’, or ‘I don't know’. A sample question was, "Is it true that women who did not breastfeed have an increased risk of developing ovarian cancer?" Each correct answer received one point, while the incorrect and ‘I don’t know’ were given zero points. Total score for this section was determined by summing up the points for all of the questions in the section and higher scores indicated greater awareness of OC risk factors among the respondents.
2.7 Sample size
The sample size for this study was estimated using the Denial equation (Ahsan et al. 2021; Meraya et al. 2022; Rao et al. 2009; Daniel and Biostatics 2013) applying the following parameters: α = 0.05 (95% confidence interval), power (1-β) = 0.80, and a 50% response distribution. A 50% response distribution was chosen as a conservative estimate in the absence of prior prevalence data, ensuring maximum sample size and statistical power. The formula used to calculate the sample size was:
where Z(1−α/2) is the standard normal variate (1.96 for 5% type 1 error, p < 0.05), ‘d’ is the absolute error or precision (0.05), and ‘P’ is the expected prevalence. The calculated sample size was cross-verified using OpenEpi (version 3.01), considering a population size of one million, a finite population correction factor, a 5% confidence limit, a design effect of 1, and a minimum sample size of 384 (Sullivan et al. 2009). To account for potential non-response and missing data, an additional 15% was added to the sample size, bringing the final target sample to approximately 442 participants. The chosen parameters and methodology align with similar epidemiological studies conducted in the region, supporting the robustness of the sample size determination.
2.8 Data collection
Data for the study were collected through a web-based survey. Volunteer data collectors were recruited by announcing the study in student groups within the College of Pharmacy, Jazan University. Five senior female interns volunteered to assist with the data collection and signed consent forms confirming that their participation was voluntary and unpaid. They received one day of training from the authors. The data collectors disseminated the survey invitation links through social media groups to ensure at least 100 participants per data collector. Regular reminders were sent until the minimum calculated sample size of 385 was achieved. The survey link remained open for responses for an additional period of three weeks to allow more responses. Data collection was monitored closely by the authors. Incomplete responses were excluded from the analysis. Out of 465 responses received, 433 were complete, yielding a response completion rate of 93%.
2.9 Informed consent
An online informed consent form was integrated into the questionnaire at the start of the survey, and participants confirmed their voluntary intent and willingness to participate by answering ‘Yes’ to a mandatory question. Only participants who consented could proceed to complete the questionnaire, and a response in form of ‘No’ to the informed consent resulted in immediate termination of the survey, and such responses are recorded as dropouts.
2.10 Statistical analysis
Data analysis was performed using SPSS version 20 (SPSS Inc., Chicago, Illinois, USA). Data from Google Forms survey was initially exported to MS-Excel, where pre-processing and coding were conducted before being imported to SPSS (Hassler et al. 2019). Descriptive statistics were used to analyze the socio-demographic information of respondents and the results were presented as frequencies, percentages, means, and standard deviations. Pearson’s correlation coefficient was applied to compare the continuous variables i.e., section scores. Additionally, a chi-square test was conducted to evaluate associations between the socio-demographic characteristics and level of knowledge of respondents, one of the outcome variables of the study. Statistical significance was set at p ≤ 0.05.
3 Results
A total of 433 out of 465 responses were analyzed in this study. The questionnaire consisted of four sections: the first section was used to collect respondents’ demographic details and medical history, the second section included questions related to the general awareness of OC, the third part assessed the knowledge of participants about OC, and the fourth section focused on assessing the awareness of participants about the risk factors associated with ovarian cancer.
Table 1 presents the results of the socio-demographics and medical history of the participants. It was predetermined in the study that only female participants would be included; hence 433 (100%) females were analyzed, while the responses of four male participants were excluded. The participants were aged between 18–60 years, with a mean age of 27.27 years (SD ± 10.12). More than three-quarters of the sample (85.2%) were aged 18–39 years, while the remaining participants were aged 40–60 years. Most of the respondents (85.9%) were Saudi nationals and were graduates and above (93.5%). More than half of the sample (65.4%) were students at Jazan University, while the remaining were either employed in private or public sectors, with 9.7% being unemployed. Similarly, more than half of the participants (64.2%) were residents of urban areas and a majority (63.7%) were single. Most respondents reported no history of communicable (75.6%) or non-communicable diseases (92.5%).
Tables 2, 3, and 4 provide the descriptive statistics of the participant's responses, presented as frequency distributions. Cronbach’s Alpha test was performed to test the internal reliability of each section of the prepared questionnaire, yielding acceptable to good reliability scores (alpha = 0.794, 0.738, and 0.816, respectively). Table 2 outlines the participants’ responses to questions assessing their general awareness of ovarian cancer. Interestingly, lesser proportion of the participants were aware of OC and its impact (27%), were aware of importance of being educated about OC (23.1%), understood the significance of regular health check-ups (9.9%), were familiar with the early symptoms of OC (19.2%), and knew about the screening tests and procedures for OC detection (15.5%), as they responded ‘yes’ to these questions. These responses reflect a limited level of awareness among the participants regarding OC. On the contrary, more than two-thirds of participants demonstrated a low level of awareness, as they responded ‘no’ or ‘I don’t know’ to these questions.
Table 3 presents the participants’ responses to questions assessing their knowledge about OC. A notable proportion of participants indicated good level of knowledge when they were asked questions about the possibility of early diagnosis of OC (51.3%) and importance of increased awareness of the OC symptoms leading to quicker diagnosis (64.4%). However, lower and varying levels of knowledge were observed for other questions of this section as high percentage of participants lacked proper knowledge about the diagnosis of OC in its early stages (85.7%), detection of OC through Pap smear test (89.3%), early-stage OC patients being symptomatic (73.7%), prolonged lower back pain as possible symptom of OC (71.6%), prolonged pelvic pain as possible indication of OC (69.2%), persistent pain the abdomen as possible indication of OC (68.1%), treatment process of OC (82.4%), and persistent bloating as a common symptom of OC (88%) as they chose ‘incorrect’ or ‘I don’t know’ responses to the respective questions.
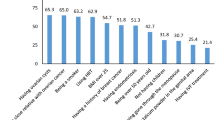
Table 4 shows participant’s responses to the questions assessing their awareness of risk factors associated with OC. Low to poor levels of awareness were observed in the participants about the OC risk factors associated as a few only responded ‘yes’ to the questions of this section. A high percentage of participants demonstrated poor awareness as they selected ‘incorrect answer’ or ‘I don’t know’ to questions asking awareness about the frequency of OC risk (76.7%), risk of OC in women who did not breastfeed (73.2%), correlation between height and OC (81.0%), risk of OC in women who had menopause (70.5%), risk of OC in women having a family history of breast cancer (87.5%), risk of development of OC with age (72.7%), risk of OC in women who have never been pregnant (81.8%), and risk of OC in patients who have undergone hormone replacement therapy (76.9%).
Table 5 categorizes general awareness, knowledge, and risk factor awareness scores based on Bloom’s cut-off point criteria (Preedy et al. 2010). According to these criteria, scores below 60% were categorized as poor, scores between 60% and less than 80% were categorized as moderate, and scores of 80% and above were categorized as good (Sullivan et al. 2009). Regarding general awareness, only a small percentage of participants (9.5%) exhibited good awareness, while the rest had either moderate (5.5%) or poor (85%) awareness. Similarly, for knowledge about OC, very few participants (2.5%) had good knowledge, with the majority displaying either moderate (8.3%) or poor (89.1%) knowledge. A vast majority (86.1%) also demonstrated poor awareness of risk factors and complications associated with OC. These findings concluded that a large proportion of the sample population lacked adequate awareness and knowledge about OC, its risk factors, and associated complications.
Table 6 presents the results of cross-tabulations between participants’ socio-demographics and their knowledge categories. Participants’ knowledge was significantly associated with age group (χ2 = 14.379; p < 0.05), nationality (χ2 = 22.334; p < 0.05), and occupation (χ2 = 31.767; p < 0.05). However, no statistically significant associations were found between participants’ knowledge and their place of residence, education level, or marital status.
Table 7 summarizes the results of the correlation between the scores of different scales. Significant positive correlations were observed between the average awareness score and the average knowledge score (r = 0.600; p < 0.01), between the average awareness score and the risk factor awareness score (r = 0.515; p < 0.01), and between the average knowledge score and the risk factor awareness score (r = 0.634; p < 0.01). These findings suggested that an increase in one score was associated with increase in the other scores.
4 Discussion
The findings of this study provided critical insights into the level of awareness and knowledge about the OC among the general population of the Jazan province, Saudi Arabia. Despite advancements in medical care and increasing global awareness efforts, a significant knowledge gap persists regarding OC, its risk factors, and early warning signs within the study population. These findings were consistent with the previous studies conducted in other regions, both locally and globally, underscoring the universal challenges in promoting OC awareness (Sabi et al. 2021). Only 9.5% of participants demonstrated good general awareness of OC, and an even smaller proportion (2.5%) exhibited good knowledge of the disease. Alarmingly, a significant majority (86.1%) of participants were unaware of the risk factors associated with OC. These statistics point to an urgent need for targeted public health campaigns and educational interventions to improve understanding of OC.
This study also revealed that the respondents having bachelor degree or above showed good to moderate knowledge about the disease, suggesting that education plays a vital role in disseminating health information. This observation aligned with global findings, including a study conducted by the World Ovarian Cancer Coalition in Toronto, Canada involving 1531 women from 44 nations, found that an average of 69.1% of women were unaware of OC before their diagnosis, with unawareness rates ranging from 50.9% in Hungary to 86.4% in Brazil (Reid et al. 2021). It emphasizes the urgent need to enhance public knowledge about OC risks and provides valuable insights for general practitioners and health educators to develop future awareness, prevention, and screening programs (Fallowfield et al. 2010).
In the western region of Saudi Arabia, a study analyzed 90 out of 119 individuals with OC and found that the majority of the patients were older than 40 years. Out of 90 tumors studied, 67 (74.44%) were at advanced stages (II-IV), and 54 (60.0%) were bilateral (Aga et al. 2022). Similar research on Malaysian women revealed that the participants had minimal awareness of the OC risk factors, highlighting the need for increased public education about OC risks and importance of equipping the health professionals with relevant information for future awareness, prevention, and screening campaigns (Elshami et al. 2022). The results of this study also aligned with a cross-sectional study conducted in Riyadh, Saudi Arabia, involving 200 women, which assessed awareness and attitude towards the screening of OC among women and revealed that a small percentage had a strong understanding of OC and its screening methods (Alhedyani et al. 2016). This consistency highlighted the global relevance of the issue, suggesting that cultural and regional differences may not significantly impact awareness levels.
The incidence of OC varies across different regions, with the highest rates observed in Europe and North America, while comparatively lower rates are reported in Asia and the Middle East (Che and Yin 2025; Wang et al. 2024; Wei et al. 1988). However, recent epidemiological data indicated a rising trend in the OC cases in Saudi Arabia which might be attributed to multiple factors, including changes in lifestyle, reproductive patterns, and dietary habits. In Saudi Arabia, OC is among the top ten cancers affecting women (Balkhy et al. 2022; Almohammadi 2022; Yousif et al. 2019). One significant contributor to the increasing incidence of OC might be a shift in the reproductive behaviors, with women increasingly delaying childbirth, having fewer children, and reducing duration of breastfeeding (Jordan et al. 2012; Zografos et al. 2004; Ovarian Cancer Risk Factors n.d.). All these factors are associated with a higher risk of OC owing to the increased lifetime exposure to ovulation cycles. Additionally, growing use of hormone replacement therapy (HRT) among postmenopausal women might also be influencing the observed trends (Lee et al. 2023).
Dietary habits in Saudi Arabia have also undergone substantial transformation over last few years, moving from traditional diets rich in whole grains, pulses, and plant-based foods to a more Westernized diet high in processed and high-fat foods. Previous studies have shown that the phytoestrogen-rich diets, such as those containing soy and soy-derived products, whole grains, and legumes, are associated with a lower incidence of hormone-sensitive cancers, including the OC (Torrens-Mas and Roca 2020). A reduction in the intake of these protective dietary components might be contributing to an increased OC risk in the general population. Furthermore, improvements in the healthcare infrastructure and cancer awareness programs in Saudi Arabia might be leading to an increased OC detection rate, contributing to an apparent rise in confirmed cases. Increased accessibility of diagnostic tests had facilitated early OC detection and more frequent diagnoses.
To the best of the authors’ knowledge, this study is the first in the Jazan province to assess both the general populations’ knowledge about OC and their awareness of its potential risk factors. It emphasizes the need of educating the healthcare professionals about the importance of patient-centered communication and health education regrading OC. Enhanced physician–patient interactions could bridge the gaps in knowledge and encourage early detection and prevention. Furthermore, incorporating OC awareness into the national health policies and leveraging media campaigns could significantly impact the understanding of general population of this critical issue.
Early detection of OC remains challenging owing to its asymptomatic nature in early stages and lack of knowledge, awareness and routine screening recommendations for the general population. OC screening is particularly important for high-risk individuals, such as those with a family history of OC or BRCA1/BRCA2 gene mutations (Huber et al. 2020; Hall et al. 2016; Amin et al. 2020). Women with a family history of OC may undergo BRCA1/BRCA2 genetic testing to determine the susceptibility and those with mutations in these genes may consider risk-reducing interventions, such as increased surveillance or prophylactic surgery. The common screening methods for OC include the CA125 blood test which is a cancer antigen often elevated in the blood of individuals with OC (Charkhchi et al. 2020; Scholler and Urban 2007). It is one of the most commonly employed screening tools for high-risk individuals, however it lacks specificity as the elevated CA125 levels can also occur in benign conditions such as endometriosis and pelvic inflammatory diseases. This test however is most useful in monitoring the progression of the disease and treatment response rather than a stand-alone diagnostic tool. Other diagnostic methods include the transvaginal ultrasound (TVUS) which is an imaging technique that helps in the detection of abnormalities in ovary including cysts and tumors (Nagell and Hoff 2013; Thaker et al. 2023). However, it is not definitive in the diagnosis of OC, and can be used in conjunction with other tests. Another method is the assessment of Risk of Malignancy Algorithm (ROMA) which combines the CA125 and HE4 (human epididymis protein 4) levels along with the menopausal status to determine the risk of ovarian malignancy (Gorp et al. 2011; Anton et al. 2012). This increases the accuracy and specificity of the detection compared to CA125 test alone.
The high standards of healthcare system in Saudi Arabia allows OC screening in all major hospitals and diagnostic centers across the kingdom including the CA125 and TVUS. Screening is generally recommended for high-risk individuals rather than for the general population owing to the lack of specificity of CA125 test. Additionally, Saudi Arabia has been emphasizing on developing awareness programs encouraging women at high risk to undergo genetic testing for BRCA1/BRCA2 mutations (Abulkhair et al. 2018; Alghamdi et al. 2014). Although, there is no nationwide routine OC screening program, but both public and private hospitals offer screening options for high-risk patients. The Saudi Ministry of Health (MoH) and institutions such as King Faisal Specialist Hospital and Research Centre (KFSHRC) promote awareness and facilitate access to the early detection services of OC.
Appropriate awareness programs targeting women in the Jazan province should be developed and emphasized addressing the key risk factors of OC such as age, family history, hormonal replacement therapy, and reproductive history. Women posing any of these risk factors should be encouraged to undergo the screening procedure to rule-out the disease. Additionally, OC awareness can also be integrated into the educational curriculums at schools and higher educational institutions to foster knowledge among younger generations. Leveraging social media and online tools to reach younger, digitally active demographics while also addressing gaps in digital accessibility for older populations. Organized screening initiatives should be established to ensure early detection of OC in high-risk groups, particularly the postmenopausal women and those with a family history of OC or related disorders. Longitudinal studies must be conducted to assess the impact of educational campaigns on OC awareness and to investigate the potential cultural and socioeconomic determinants influencing knowledge levels among general population.
5 Limitations of the study
There are several limitations to this study, as its cross-sectional design did not allow for the establishment of causal relationships. Additionally, the volunteer online survey approach carried a substantial risk of selection bias. The test–retest reliability of the questionnaire could not be confirmed, as tracing and re-engaging the same respondents was challenging. Moreover, the invitation link to participate in the survey was distributed through social media platforms, which might have excluded elderly individuals without internet access, those not active on social media, or those unfamiliar with the Google Forms. Furthermore, the use of convenience sampling method limited the generalizability of the findings to the larger population of the Jazan province. The snowball sampling technique employed might also have led to possible selection bias, and self-reported data are inherently prone to recall bias. Eventually, this study did not examine the formal or informal sources of information participants used to acquire knowledge about OC. Future research aims to expand the scope to include other regions of Saudi Arabia, with the goal of obtaining the nationwide data.
6 Conclusions
The findings of this study demonstrated that a substantial proportion of the sampled population exhibited limited knowledge of OC and inadequate awareness of its associated risk factors and potential complications. Only a small proportion of participants demonstrated good awareness or knowledge of OC, while a majority were unaware of its risk factors. These results emphasize the critical need for developing, coordinating, and implementing evidence-based educational interventions targeting the general population, with a particular emphasis on OC. Such initiatives should aim to enhance knowledge, promote early identification of risk factors, and encourage preventive behaviors. Increasing awareness among women in the Jazan region of Saudi Arabia is especially important, given the observed knowledge gaps. Structured, culturally appropriate training and awareness programs are essential to improve women’s health outcomes and to foster their active engagement in educational campaigns related to OC prevention, risk reduction, and early detection.
Data availability
All the data associated with this study are included in the article.
References
Abulkhair O, Al Balwi M, Makram O, Alsubaie L, Faris M, Shehata H, Hashim A, Arun B, Saadeddin A, Ibrahim E (2018) Prevalence of BRCA1 and BRCA2 mutations among high-risk Saudi patients with breast cancer. J Glob Oncol 4:1–9. https://doi.org/10.1200/JGO.18.00066
Aga SS, Jaha R, Khan R, Junaydi D, Hakami A, Khan MA et al (2022) Detailed demographics and the prevalence of comorbidities in ovarian cancer patients in western region of Saudi Arabia. J Nat Sci Med 5:254–261. https://doi.org/10.4103/jnsm.jnsm_158_21
Ahsan W, Syed NK, Alsraeya AA, Alhazmi HA, Najmi A, Al Bratty M et al (2021) Post-vaccination survey for monitoring the side effects associated with COVID-19 vaccines among healthcare professionals of Jazan province, Saudi Arabia. Saudi Med J 42:1341–1352. https://doi.org/10.15537/smj.2021.42.12.20210576
Alghamdi I, Hussain I, Alghamdi M, Alghamdi M, Dohal A, El-Sheemy M (2014) Incidence rate of ovarian cancer cases in Saudi Arabia: an observational descriptive epidemiological analysis of data from Saudi Cancer Registry 2001–2008. Int J Womens Health 6:639–645. https://doi.org/10.2147/IJWH.S63636
Alghamdi AG, Algharsan FA, Alzahrani RA, Alghamdi RH, Alzahrani AA, Alzahrani YK, Hussain MF (2024) Knowledge about breast cancer and barriers to screening among Saudi women in Al-Baha Region. Asian Pac J Cancer Prev. 25(3):977–986. https://doi.org/10.31557/APJCP.2024.25.3.977
Alhedyani NA, Alsaigh A, Alrumayyan L, Bohligah N, Aldhawi N, Alhedyani AA et al (2016) Women’s awareness and attitude toward screening of ovarian cancer in Riyadh, Saudi Arabia. Int J Adv Res 4:2189–2198. https://doi.org/10.21474/IJAR01/2635
Almohammadi NH (2022) The pattern of gynecological malignancies in Al-Madinah Al-Munawarah region, Saudi Arabia. Saudi Med J 43(3):283–290. https://doi.org/10.15537/smj.2022.43.3.20210888
Amin N, Chaabouni N, George A (2020) Genetic testing for epithelial ovarian cancer. Best Pract Res Clin Obstet Gynaecol 65:125–138. https://doi.org/10.1016/j.bpobgyn.2020.01.005
Anton C, Carvalho FM, Oliveira EI, Maciel GA, Baracat EC, Carvalho JP (2012) A comparison of CA125, HE4, risk ovarian malignancy algorithm (ROMA), and risk malignancy index (RMI) for the classification of ovarian masses. Clinics (Sao Paulo) 67(5):437–441. https://doi.org/10.6061/clinics/2012(05)06
Assiry A, Alshahrani S, Banji D, Banji OJF, Syed NK, Alqahtani SS (2022) Public awareness of chronic kidney disease in Jazan Province, Saudi Arabia-A cross-sectional survey. Healthcare 10(8):1377. https://doi.org/10.3390/healthcare10081377
Balkhy AL, Saleh ER, Jabali HI, Al-Jifree HM, Alwazzan AB (2022) Demographic features, clinical characteristics, and prognostic factors of non-epithelial ovarian tumors at Princess Noorah Oncology Center, National Guard Hospital, Jeddah, Saudi Arabia. Saudi Med J 43(2):208–212. https://doi.org/10.15537/smj.2022.43.2.20210433
Beaton DE, Bombardier C, Guillemin F, Ferraz MB (2000) Guidelines for the process of cross-cultural adaptation of self-report measures. Spine 25(24):3186–3191. https://doi.org/10.1097/00007632-200012150-00014
Browne RH (1995) On the use of a pilot sample for sample size determination. Stat Med 14(17):1933–1940. https://doi.org/10.1002/sim.4780141709
Charkhchi P, Cybulski C, Gronwald J, Wong FO, Narod SA, Akbari MR (2020) CA125 and ovarian cancer: a comprehensive review. Cancers (Basel) 12(12):3730. https://doi.org/10.3390/cancers12123730
Che M, Yin R (2025) Analysis of the global burden of ovarian cancer in adolescents. Int J Gynecol Cancer. Online ahead of print. https://doi.org/10.1016/j.ijgc.2024.101620
Cronbach LJ (1951) Coefficient alpha and the internal structure of tests. Psychometrika 16:297–334. https://doi.org/10.1007/BF02310555
da Silva IM, da Silva Nogueira TQ, Couto DN, Meira Lima PC, Bonfim NS, de Sousa IG et al (2022) Feasibility of a snowball sampling survey to study active surveillance for thyroid microcarcinoma treatment among endocrinologists and surgeons of Brazil. Braz J Otorhinolaryngol 88(Suppl 4):S163–S169. https://doi.org/10.1016/j.bjorl.2022.01.005
Daniel WW, Cross CL (2013) Biostatics: a foundation for analysis in the health sciences, 10th edn. John Wiley & Sons Inc., Hoboken (NY)
Degroot AMB, Dannenburg L, Vanhell JG (1994) Forward and backward word translation by bilinguals. J Mem Lang 33:600–629. https://doi.org/10.1006/jmla.1994.1029
Elshami M, Tuffaha A, Yaseen A, Alser M, Al-Slaibi I, Jabr H et al (2022) Awareness of ovarian cancer risk and protective factors: a national cross-sectional study from Palestine. PLoS ONE 17(3):e0265452. https://doi.org/10.1371/journal.pone.0265452
Fallowfield L, Fleissig A, Barrett J, Menon U, Jacobs I, Kilkerr J et al (2010) Awareness of ovarian cancer risk factors, beliefs and attitudes towards screening: baseline survey of 21,715 women participating in the UK collaborative trial of ovarian cancer screening. Br J Cancer 103(4):454–461. https://doi.org/10.1038/sj.bjc.6605809
Fauville G, Luo M, Queiroz AC, Bailenson JN, Hancock J (2021) Zoom exhaustion & fatigue scale. Comput Human Behav Rep 4:e100119. https://doi.org/10.1016/j.chbr.2021.100119
First Saudi Women’s Cancer Summit (n.d.) Saudi Arabia: Saudi society for internal medicine at King Abdul Aziz University [last updated 2020 Sep 17]. Available from: https://ssim.kau.edu.sa/Pages-CANCER.aspx. Accessed 24 May 2024
Global Cancer Observatory (n.d.) Cancer Today. Lyon, France: International agency for research on cancer. Ovarian cancer in Saudi Arabia. [Last updated 2021 Oct 10]. Available from: https://gco.iarc.fr/today/data/factsheets/populations/682-saudi-arabia-fact-sheets.pdf. Accessed 24 May 2024
Hall MJ, Obeid EI, Schwartz SC, Mantia-Smaldone G, Forman AD, Daly MB (2016) Genetic testing for hereditary cancer predisposition: BRCA1/2, Lynch syndrome, and beyond. Gynecol Oncol 140(3):565–574. https://doi.org/10.1016/j.ygyno.2016.01.019
Hassler AP, Menasalvas E, García-García FJ, Rodríguez-Mañas L, Holzinger A (2019) Importance of medical data preprocessing in predictive modeling and risk factor discovery for the frailty syndrome. BMC Med Inform Decis Mak 19:e33. https://doi.org/10.1186/s12911-019-0747-6
Huang J, Chan WC, Ngai CH, Lok V, Zhang L, Lucero-Prisno DE III et al (2022) Worldwide burden, risk factors, and temporal trends of ovarian cancer: a global study. Cancers 14:2230. https://doi.org/10.3390/cancers14092230
Huber D, Seitz S, Kast K, Emons G, Ortmann O (2020) Use of oral contraceptives in BRCA mutation carriers and risk for ovarian and breast cancer: a systematic review. Arch Gynecol Obstet 301(4):875–884. https://doi.org/10.1007/s00404-020-05458-w. (Erratum.In:ArchGynecolObstet.2022;305(6):1627.10.1007/s00404-021-06266-6)
Jordan SJ, Cushing-Haugen KL, Wicklund KG, Doherty JA, Rossing MA (2012) Breast-feeding and risk of epithelial ovarian cancer. Cancer Causes Control 23(6):919–927. https://doi.org/10.1007/s10552-012-9963-4
Keng SL, Abdul-Wahab SB, Chiu LB, Yusuf A (2015) Awareness of ovarian cancer risk factors among women in Malaysia: a preliminary study. Asian Pac J Cancer Prev 16:537–540. https://doi.org/10.7314/apjcp.2015.16.2.537
Lee HJ, Lee B, Choi H, Kim T, Kim Y, Kim YB (2023) Impact of hormone replacement therapy on risk of ovarian cancer in postmenopausal women with De Novo endometriosis or a history of endometriosis. Cancers (Basel) 15(6):1708. https://doi.org/10.3390/cancers15061708
Lengyel E (2010) Ovarian cancer development and metastasis. Am J Pathol 177:1053–1064. https://doi.org/10.2353/ajpath.2010.100105
Meraya AM, Ahsan W, Albratty M, Alhazmi HA, Najmi A (2022) Perception of individuals with diabetes about efficacy and safety of complementary and alternative medicines (CAM) in the Jazan Region, Saudi Arabia. Evid Based Complement Alternat Med 2022:1–8. https://doi.org/10.1155/2022/2104056
Ottevanger PB (2017) Ovarian cancer stem cells more questions than answers. Semin Cancer Biol 44:67–71. https://doi.org/10.1016/j.semcancer.2017.04.009
Ovarian Cancer Risk Factors (n.d.) American Cancer Society. Webpage available online at: https://www.cancer.org/cancer/types/ovarian-cancer/causes-risks-prevention/risk-factors.html. Accessed on March 2, 2025
Ovarian Cancer Statistics (2020) London: World Cancer Research Fund International [last updated 2022 March 23]. Available from: http://www.wcrf.org/int/cancer-facts-figures/data-specific-cancers/ovarian-cancer-statistics. Accessed 24 May 2024
Preedy VR, Watson RR (2010) 5-Point Likert scale. In: Preedy VR, Watson RR (eds) Handbook of disease burdens and quality of life measures. Springer, New York, pp 4288–4288
Rao SR, Rao PM, editors (2009) Sample Size Calculator by Raosoft, Inc. Available from: http://www.raosoft.com/samplesize.html. Accessed 24 May 2024
Reid F, Bhatla N, Oza AM, Blank SV, Cohen R, Adams T et al (2021) The world ovarian cancer coalition every woman study: identifying challenges and opportunities to improve survival and quality of life. Int J Gynecol Cancer 31(2):238–244. https://doi.org/10.1136/ijgc-2019-000983
Russo A, Calò V, Bruno L, Rizzo S, Bazan V, Di Fede G (2009) Hereditary ovarian cancer. Crit Rev Oncol Hematol 69:28–44. https://doi.org/10.1016/j.critrevonc.2008.06.003
Sabi EM, Mujamammi AHA, Abdulghani M, Almesfer YM, Alsuwaida AA, Balobaid AS et al (2021) Awareness level of cancer risk factors and warning signs and cancer campaign attendance behavior among Saudi adults in a tertiary hospital in Riyadh. Asian Pac J Cancer Prev 22(8):2421–2428. https://doi.org/10.31557/APJCP.2021.22.8.2421
Scholler N, Urban N (2007) CA125 in ovarian cancer. Biomark Med 1(4):513–523. https://doi.org/10.2217/17520363.1.4.513
Sullivan KM, Dean A, Soe MM (2009) On Academics: OpenEpi: a web-based epidemiologic and statistical calculator for public health. Public Health Rep 124:471–474. https://doi.org/10.1177/003335490912400320
Tavakol M, Dennick R (2011) Making sense of Cronbach’s alpha. Int J Med Educ 2:53–55. https://doi.org/10.5116/ijme.4dfb.8dfd
Thaker N, Dhande R, Parihar P (2023) Role of transvaginal sonography in the diagnosis of female infertility: a comprehensive review. Cureus 15(12):e50048. https://doi.org/10.7759/cureus.50048
Torre LA, Trabert B, DeSantis CE, Miller KD, Samimi G, Runowicz CD et al (2018) Ovarian cancer statistics, 2018. CA Cancer J Clin 68(4):284–296. https://doi.org/10.3322/caac.21456
Torrens-Mas M, Roca P (2020) Phytoestrogens for cancer prevention and treatment. Biology 9(12):427. https://doi.org/10.3390/biology9120427
Van Gorp T, Cadron I, Despierre E, Daemen A, Leunen K, Amant F, Timmerman D, De Moor B, Vergote I (2011) HE4 and CA125 as a diagnostic test in ovarian cancer: prospective validation of the risk of ovarian malignancy algorithm. Br J Cancer 104(5):863–870. https://doi.org/10.1038/sj.bjc.6606092
van Nagell Jr JR, Hoff JT (2013) Transvaginal ultrasonography in ovarian cancer screening: current perspectives. Int J Women’s Health 25–33. https://doi.org/10.2147/IJWH.S38347
Wang M, Bi Y, Jin Y, Zheng Z-J (2024) Global incidence of ovarian cancer according to histologic subtype: a population-based cancer registry study. JCO Glob Oncol 10:e2300393. https://doi.org/10.1200/GO.23.00393
Wei Y-F, Ning L, Xu Y-L, Ma J, Li D-R, Feng Z-F et al (2025) Worldwide patterns and trends in ovarian cancer incidence by histological subtype: a population-based analysis from 1988 to 2017. eClinicalMed 79:102983. https://doi.org/10.1016/j.eclinm.2024.102983
Yousif HM, Mohammed RA, Missawi HM, Elsawaf ZM, Albasri AA (2019) Histopathological patterns of primary malignant ovarian neoplasms in different age groups in Almadinah Almunawwarah region, KSA. J Taibah Univ Med Sci 14(1):73–78. https://doi.org/10.1016/j.jtumed.2018.11.005
Zografos GC, Panou M, Panou N (2004) Common risk factors of breast and ovarian cancer: recent view. Int J Gynecol Cancer 14:721–740
Acknowledgements
The authors gratefully acknowledge the funding of the Deanship of Graduate Studies and Scientific Research, Jazan University, Saudi Arabia, through the project number: RG24-L07.
The authors would like to thank the Pharmacy Practice Research Unit (PPRU), College of Pharmacy, Jazan University for promoting research and development activities. Authors also appreciate the volunteers (Reem Othman Alaqi, Ebtesam Badr Ali, Alaa Mohsen Abed Alhazmi, Ahlam Ebrahim Ali) and the respondents who willingly participated in this study. We are also grateful to Professor Dame Lesley Fallowfield, Brighton & Sussex Medical School, University of Sussex, UK for granting permission to use their questionnaire.
Funding
This work was funded by the Deanship of Graduate Studies and Scientific Research, Jazan University, Saudi Arabia, through the project number: RG24-L07.
Author information
Authors and Affiliations
Contributions
Conceptualization: GK, MSA, SJ; Data curation: GK, MSA, SJ; Formal analysis: MSA, WA, HM; Investigation: WA, HM, KZ, AN; Methodology: GK, MSA, SJ, WA, AK, ANQ, KAA; Project administration: HM, KZ, AN, AK; Resources: HM, KZ, AN, AK; Software: GK, MSA, SJ, WA; Supervision: HM, KZ, AN, AK; Validation: HM, KZ, AN, AK, ANQ, KAA; Roles/Writing—original draft: GK, MSA, SJ, WA; and Writing—review & editing: HM, KZ, AN, AK, ANQ, KAA.
Corresponding authors
Ethics declarations
Ethics declaration
The methodology, questionnaire, and informed consent procedures involved in the study were reviewed and approved by the Institutional Research Review and Ethics Committee (IRREC), Jazan University. Approval was granted under reference no. REC-44/06/449 dated January 2, 2022. The research was initiated only after receiving ethical clearance. The study adhered to the ethical principles of the Helsinki declaration for medical research involving human beings.
Conflict of interest
None declared.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Khuwaja, G., Ansari, M.S., Javed, S. et al. Assessment of knowledge and awareness about ovarian cancer and its risk factors among women in Jazan, Saudi Arabia: a cross-sectional study. Saudi Pharm. J. 33, 1 (2025). https://doi.org/10.1007/s44446-025-00002-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s44446-025-00002-w