
Abstract
Hysterosalpingography (HSG) is a minimally invasive procedure that can be painful. This study aimed to examine the impact of a tailored training program on anxiety and perceived pain intensity in infertile women undergoing HSG. This research was a clinical trial involving 86 infertile women who were candidates for HSG and conducted at the radiology department of the Royan Infertility Center in Tehran, Iran, between November 22, 2021, to March 11, 2023.The participants were divided into two groups:43 women in the intervention group and 43 women in the control group. The randomization of the samples was carried out using a random number table. The women in the intervention group received two face-to-face group training sessions. Data were collected using valid questionnaires. Additionally, the heart rate and blood pressure of the participants were recorded. Data analysis showed the training intervention was significantly associated with reducing anxiety levels, perceived pain, systolic blood pressure, diastolic blood pressure, and heart rate in women undergoing HSG (p < 0.05). These findings support the use of structured training interventions to improve the overall experience and outcomes for patients undergoing HSG.
Trial Registration Number: IRCT20150905023897N4.
Similar content being viewed by others

Introduction
Infertility is defined as the inability to achieve pregnancy after 12 months of regular sexual intercourse without contraception. It is estimated that approximately 8 to 12% of couples of reproductive ages worldwide experience infertility1. In various studies, the rate of infertility has been reported to vary, ranging from approximately 6.6–26.4% in industrialized countries. Causes of female infertility encompass disorders affecting the fallopian tubes, uterus, cervix, and ovaries. Specifically, fallopian tube disorders are responsible for approximately 30–40% of infertility cases2. In Iran, the lifetime prevalence of infertility is reported to be 11.3%3. Hysterosalpingography (HSG) is among the various methods used for evaluating infertile women4,5. HSG is a conventional and widely used method for early diagnosis of infertility, especially the causes associated with fallopian tube abnormalities6,7,8. This method is minimally invasive but may be associated with complications such as allergic reactions, pain, abdominal cramps, and rarely, shock9. Pain experienced during and after HSG impairs women’s ability to cooperate and may hinder the optimal performance of the procedure5. In addition to anatomical and physical reasons, psychological factors such as depression and anxiety have been reported as influencing factors in the perception of pain during this procedure10. Studies indicate that preoperative anxiety significantly impacts perceived pain during and after surgery, as well as during minimally invasive procedures11,12. Increased anxiety levels are associated with higher stress intensity and a lower pain tolerance threshold. Therefore, reducing anxiety in patients undergoing these procedures is crucial to enhance their experience and outcomes5,11,13.
Some research supports the benefits of psychological psychotherapy, education and counseling in reducing psychological symptoms such as anxiety and depression in infertile women and patients undergoing painful procedures15,16,17,18. Considering the necessity of alleviating pain and anxiety in HSG candidates, particularly through non-pharmacological methods and patient education, this study was designed to assess the impact of a training program on anxiety and perceived pain intensity in infertile women undergoing HSG at the Royan Research Institute in Tehran.
Methods
Trial design
This study was a two-phase, double-blind randomized trial, where neither the participants nor the teaching researcher knew the group assignments. It was conducted at the radiology department of the Royan Infertility Center in Tehran, Iran, from November 22, 2021, to March 11, 2023. This trial adhered to the ethical guidelines of the 1975 Declaration of Helsinki, and ethical approval was obtained from the Ethics Committee of Tarbiat Modares University, Tehran, Iran, prior to the start of the study on November 1, 2021 (IR.MODARES.REC.1401.144). Furthermore, it was registered in the Iranian Registry of Clinical Trials on November 9, 2021 with the registration number IRCT20150905023897N6.
Participants
The study included Iranian infertile women who met specific inclusion criteria. These criteria were: willingness to participate, aged between 20 and 45 years, ability to speak Persian, literacy in reading and writing, absence of known anxiety disorders or other mental illnesses affecting anxiety, and no history of prior HSG procedures. The exclusion criteria included the patient’s decision to withdraw from the study, inability to complete the hysterosalpingography procedure for any reason, or the presence of tubal or uterine abnormalities, such as cervical stenosis or hydrosalpinx, which could cause severe pain during the HSG process (Fig. 1). According to the findings of Bal et al.19, with a 95% confidence interval and 80% test power, the sample size was calculated to be 43 women per group.
Alpha is the probability of type 1 error and beta is the probability of type 2 error. A type I error, or false positive, is the error of rejecting a null hypothesis when it is true, and a type II error, or false negative, is the error of accepting a null hypothesis when the alternative hypothesis is true. α = 0.05, Z α/2 = 1.96, β = 0.2, Zβ=1.28.
The power of test is the probability of rejecting the null hypothesis when it is false. in other words; it is the probability of avoiding a type II error.1-β = 0.8.
Effect size measures the amount of difference an intervention makes. The effect size tells how meaningful the difference between groups is20.
µ1, µ2: means of each sample. (µ1-µ2)/σ = 0.70.

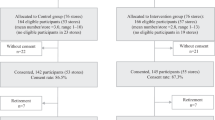
The consort flowchart.
After obtaining written permission and referring to the radiology department of Royan Research Institute, the researcher selected 86 infertile women who met the inclusion criteria. The randomization of the samples into groups was performed using a random number table. Each group was intended to consist of 43 individuals. The data collection tools included the following:
-
Demographic information questionnaire.
-
Pain visual analog scale (VAS).
-
Spielberg’s trait - situational anxiety questionnaire (STIA).
-
Questionnaire of patients’ awareness of hysterosalpingography (researcher made).
-
Sphygmomanometer for blood pressure.
-
Pulse meter to measure heart rate.
The demographic information questionnaire consisted of 40 questions, and its validity and reliability were assessed. The questions covered various aspects including: name and surname, residence and workplace address, phone number, duration of marriage, education level, economic status, ethnicity, history of surgery, physical activity status, height and weight (BMI), menstrual cycle status, type and history of infertility and pregnancy status.
Visual analog scale (VAS)
The Pain Visual Analog Scale (VAS) is a linear scale with ten numbers used to assess pain intensity. In this scale, zero represents no pain. Scores from 4 to 6 indicate moderate pain, while scores from 7 to 10 indicate severe pain. Patients indicate the number on the scale that corresponds to their perceived pain intensity21. The validity and reliability of this questionnaire have been confirmed in Iran by Rezvani et al. in 201222 (Reliability: r = 0.94, P = 0.001, construct validity: with correlations ranging from 0.71 to 0.78).
State trait anxiety inventory (STAI)
The State Trait Anxiety Inventory (STAI) is a 40-question self-report questionnaire used to assess both state (obvious) and trait (hidden) anxiety. The first 20 questions focus on current feelings of anxiety, while the second 20 questions assess enduring aspects of anxiety. Responses are scored on a Likert scale ranging from “completely agree” to “completely disagree”23. The STAI demonstrated reliability, with an alpha coefficient of 0.84 for the trait anxiety scale and 0.706 for the state anxiety scale24. In addition, Panahi et al.25 confirmed the reliability and validity of the Iranian version of the STAI questionnaire. According to their findings, scores on the STAI are categorized as follows: A score of 40 to 79.9 indicates mild anxiety, 80 to 119.9 indicates moderate anxiety, and a score of 120 to 160 indicates severe anxiety.
Questionnaire of patients’ awareness of hysterosalpingography
This researcher-made questionnaire was designed by reviewing similar research and authentic articles aligned with the research objectives. After thorough review of literature and studies, 27 questions with 4 options each were formulated. Both qualitative and quantitative methods were employed to establish content validity. For qualitative validation, the questions were reviewed by 10 experts including radiologists, obstetricians and gynecologists, midwifery specialists with master’s degrees, and epidemiology specialists. Their feedback focused on correcting grammar, refining phrasing, and ensuring the appropriate placement of content within the questionnaire.
To ensure quantitative content validity, the Content Validity Ratio (CVR) and Content Validity Index (CVI) were employed, resulting in the removal of 3 questions from the initial set. Face validity was assessed using a sample of ten infertile women, who evaluated the questionnaire items for clarity, relevance, and importance to their condition. Based on their feedback, 6 additional questions were included. The internal consistency of the questionnaire was assessed using Cronbach’s alpha coefficient, which was found to be 0.92 for the 18 items, indicating high reliability. Additionally, test-retest reliability was evaluated by having thirty infertile women complete the questionnaire twice with a 10-day interval. The Intraclass Correlation Coefficient (ICC) for all questions was found to be acceptable at 0.82, indicating good stability over time.
Intervention (two group training sessions)
The education program, which included engaging PowerPoint presentations and videos, was developed in collaboration with experts in midwifery, radiology, and gynecology. Prior to the main study, a pilot study was conducted to assess the educational needs of the participants and refine the content of the educational intervention accordingly. Based on the findings from the pilot study, adjustments were made to enhance the educational content and ensure it effectively addressed the specific needs and concerns of participants undergoing HSG.
During the first visit, which took place one day before the HSG, women in the intervention group were directed to a specially prepared room for group training. They were organized into small groups of 3–5 individuals and received a 30-minute session led by a postgraduate midwife (the lead researcher). The training covered several topics including the definition and purpose of HSG, the timing and preparation required before the procedure, the benefits of HSG in diagnosing infertility, potential side effects, and a question-and-answer session. Additionally, participants were provided with the center’s routine brochure for further information.
During the second visit, which occurred one the day of the HSG procedure, the intervention group received an additional 30-minute educational session focusing on the practical aspects of how HSG is performed, the procedural steps involved, and another opportunity for questions and answers. Thirty minutes after the educational intervention, participants completed the questionnaire and were then directed to the imaging room.
Throughout the training sessions, women had the opportunity to ask questions to the researcher and exchange information with each other. The intervention group received two face-to-face group training sessions along with the center’s routine brochure, whereas the control group only received the center’s routine training brochure.
Thirty minutes after the educational intervention, prior to undergoing HSG, both the intervention and control groups completed anxiety and awareness questionnaires specific to HSG, as well as the Pain Visual Analog Scale (VAS) and State Trait Anxiety Inventory (STAI) to assess pain intensity. After completing these assessments, all participants were directed to the imaging room to proceed with the HSG procedure.
Immediately and 30 min after undergoing HSG, both groups again completed STAI and VAS questionnaires to assess their current anxiety levels and pain perception post-procedure. Additionally, their blood pressure and heart rate were measured and recorded both before and after undergoing HSG to evaluate the physiological responses to the procedure. All participants also completed the Demographic information questionnaire.
Statistical analysis
Statistical analyses were conducted using SPSS Version 22 (SPSS Inc., Chicago, IL, USA). The normal distribution of variables was assessed using the Kolmogorov-Smirnov test. Continuous variables were presented as mean ± standard deviation (SD), while categorical variables were presented as frequencies and percentages.
Student’s t-tests were employed to compare continuous variables between the intervention and control groups. Analysis of Covariance (ANCOVA) and Multivariate Analysis of Covariance (MANCOVA) were utilized for comparisons between groups while controlling for potential confounding variables. A significance level of p < 0.05 was considered statistically significant for all analyses.
Results
The study included 86 infertile women who were randomly assigned to either the intervention or control group. The participants had a mean age of 32.20 ± 6.30 years and a mean Body Mass Index (BMI) of 24.10 ± 3.50. Upon analysis, the distribution of age, BMI, duration of marriage, menarche age, bleeding duration, and occupation status did not show statistically significant differences between the intervention and control groups (P > 0.05) (Table 1). However, there was a statistically significant difference in the duration of infertility between the intervention and control groups (P < 0.05).
The scores for awareness of hysterosalpingography in the intervention group showed a significant increase following face-to-face training. Additionally, the level of anxiety in the intervention group significantly decreased both before undergoing HSG, immediately after, and 30 min later (P < 0.05) (Table 2).
The level of anxiety in the intervention group was significantly reduced before HSG, immediately after, and 30 min later (P < 0.05) (Table 2).
Comparison of the pain levels before, immediately after, and 30 min after HSG in both control and intervention groups showed that there was no significant difference in the pain levels before HSG between the two groups (6.50 ± 1.50 vs. 6.40 ± 1.20, P = 0.82). However, the pain levels immediately after HSG and 30 min later in the intervention group decreased significantly (P = 0.001), as shown in Table 3.
Independent t - test was used to compare systolic blood pressure in the control and intervention groups. The results showed that there was no significant difference between the systolic blood pressure in the intervention and control groups before and immediately after the HSG test. However, there was a significant difference between the two groups 30 min after the HSG test, with systolic blood pressure being significantly reduced in the intervention group (P < 0.05, Table 4). Furthermore, there was no significant difference in diastolic blood pressure between the control and intervention groups before HSG. However, immediately after HSG and 30 min later, diastolic blood pressure significantly decreased in the intervention group compared to the control group (Table 4).
Comparison of heart rate between the two groups showed a significant decrease 30 min after the HSG test in the intervention group (Table 4).
Discussion
HSG is generally considered a safe procedure, but it can induce pain that exacerbates anxiety and fear in patients. The pain experienced during and after HSG can significantly impact women’s ability to cooperate with the procedure and their willingness to undergo similar diagnostic tests in the future14. This negative experience may deter patients from seeking necessary medical evaluations or treatments, highlighting the importance of managing pain and anxiety effectively during HSG to optimize patient comfort and compliance. Therefore, the present study aimed to investigate the impact of a structured training program on anxiety and perceived pain intensity during the HSG procedure in infertile women. Among the demographic variables assessed, only the duration of infertility showed a significant difference between the intervention and control groups (p < 0.05). This aligns with findings from Daniyali’s study, where similar results were observed. In Daniyali’s research, there was no statistically significant difference between the intervention and control groups in terms of demographic characteristics such as age, gender, duration of illness, and education level25. These findings highlight the comparability of baseline demographic factors between groups, thereby enhancing the study’s internal validity by minimizing potential confounding variables.
High levels of anxiety have been linked to decreased pain tolerance26. Face-to-face training conducted before medical procedures is generally recognized as a preventive measure to reduce patient anxiety and pain. According to the findings of this study, increasing awareness through face-to-face training significantly reduced anxiety and perceived pain among infertile women. Specifically, the average anxiety score in the intervention group was significantly lower before HSG, immediately after, and 30 min after the procedure. In line with this study’s findings, Guvens et al.27 conducted a study involving 105 infertile women in intervention and control groups. They found that after receiving training and counseling, there was a significant decrease in anxiety and pain levels in the intervention group compared to the control group. Erkilinç et al.13 investigated the effect of a preoperative informational video on anxiety levels of patients undergoing HSG. They observed that women who received video training had lower levels of anxiety, highlighting the effectiveness of visual educational tools in anxiety reduction. Moreover, Lee et al.28 concluded from their study that preoperative educational interventions effectively informed patients undergoing surgery, resulting in reduced pain, anxiety, and fear post-surgery. This emphasizes the role of comprehensive education in preparing patients mentally and emotionally for medical procedures. State anxiety levels depend on both individual traits and the specific stressors encountered29. Educating patients can normalize women’s anticipations of the procedure, potentially lowering their levels of pain and anxiety.
In our study, women in both groups, particularly the control group, reported high pain levels before the HSG examination, likely due to anxiety, fear of the unknown, and prior accounts of others’ painful experiences26,27. Since there is a direct relationship between fear and anxiety with the amount of pain, these people are worried before HSG. They have “fear of the unknown” because the environment, people and procedure are unfamiliar to them. Especially since the HSG procedure is called “surgery”, before the HSG most people think that a difficult and heavy surgery is ahead and they are worried and this fear affects the amount of pain30. Emotional stress, previous negative medical experiences, and individual pain sensitivity also contributed to this heightened perception of pain. However, the intervention group, which received educational training, experienced significantly reduced pain immediately and 30 min after the HSG compared to the control group. However, the findings from Fianza et al. study26, which investigated the effectiveness of educational and counseling interventions in reducing anxiety among women undergoing HSG, were contrary to our results as they did not observe a reduction in pain scores25,31. On the other hand, Balic et al. study32 aligned with our findings by demonstrating that counseling can effectively reduce anxiety and pain levels in patients. Their research indicated that pre-procedure counseling before amniocentesis can mitigate pain and anxiety among mothers. These findings suggest that various forms of education can enhance awareness and understanding of diagnostic procedures, potentially influencing pain and anxiety outcomes positively. Additionally, such educational interventions foster mutual support and understanding among peers facing similar challenges28,32. Surgical and invasive diagnostic-therapeutic procedures typically induce stress in patients, triggering both psychological and physiological reactions in the body33. Training interventions aimed at managing stress manifest in various forms, with stress control being fundamental for regulating vital signs in individuals. The findings of this study indicated a significant decrease in both systolic and diastolic blood pressure 30 min after HSG in the intervention group. Additionally, the heart rate of women in the intervention group decreased 30 min after the HSG procedure, compared to the control group. The findings of Moghadam et al. study33, which explored the impact of stress stimuli on blood pressure and heart rate among coronary artery patients compared to healthy individuals (n:163) based on excitement-seeking levels, are consistent with our study. They concluded that induced stressors correlate with increased blood pressure and heart rate and decreased overall health, suggesting that mood induction methods could potentially enhance physical health outcomes. Similarly, Babaei et al. (34) reported in their study that the mean systolic and diastolic blood pressure significantly decreased in the test group following an educational intervention, aligning with the results of our study. These studies collectively highlight the potential benefits of educational interventions in managing physiological responses such as blood pressure and heart rate in medical contexts.
Limitations & strengths
A limitation of the present study was the short time interval between the training sessions and the HSG procedure, which prevented the investigation of long-term effects of the training intervention. In addition, the difference in the duration of infertility between the intervention and control groups can be considered a limitation because it introduces a potential confounding factor. In future studies, matching participants on relevant demographic variables or using statistical adjustments during analysis can mitigate the impact of baseline differences, such as the duration of infertility, and further enhance the reliability of study findings.
One of the strengths of this study was the incorporation of group training. Group training enables participants to learn not only from the instructor but also from other patients facing similar challenges, which fosters stronger social relationships and emotional connections among individuals with shared experiences. The findings of this research can be applied in clinical settings by incorporating face-to-face training sessions, provided by midwives in infertility centers, as a routine part of infertility treatment services.
Outcome
Primary outcome included increased awareness, decreased anxiety levels, and reduced pain intensity in the intervention group. Secondary efficacy outcome comprised significant changes in intervention groups’ systolic and diastolic blood pressure, as well as heart rate, measured 30 min after the HSG procedure.
Conclusion
Our study indicates that a structured face-to-face training program can potentially benefit infertile women undergoing HSG by reducing anxiety, perceived pain, and lowering physiological responses such as blood pressure and heart rate. This approach, delivered through affordable means of group sessions, not only educates participants about the procedure but also fosters mutual support and understanding among peers facing similar challenges. These findings highlight the importance of comprehensive patient education in improving diagnostic and minor surgical experiences and outcomes, advocating for its integration into routine clinical practice to enhance overall patient experience, care and satisfaction.
Data availability
The data sets used and analyzed for the current study are available upon reasonable request of the corresponding author Dr. Shahideh Jahanian (shahideh.jahanian@modares.ac.ir).
Abbreviations
- HSG:
-
Hysterosalpingography
- VAS:
-
Visual Analog Scale
- STIA:
-
Spielberg’s trait-situational anxiety questionnaire
- SD:
-
Standard Deviation
References
Vander Borght, M. & Wyns, C. Fertility and infertility: definition and epidemiology. Clin. Biochem. 62, 2–10 (2018).
La Fianza, A. et al. Effectiveness of a single education and counseling intervention in reducing anxiety in women undergoing hysterosalpingography: a randomized controlled trial. The Scientific World Journal. ;2014. (2014).
Abangah, G., Rashidian, T., Nasirkandy, M. P. & Azami, M. A meta-analysis of the prevalence and etiology of infertility in Iran. Int. J. Fertility Steril. 17 (3), 160 (2023).
Omidiji, O. A., Toyobo, O. O., Adegbola, O., Fatade, A. & Olowoyeye, O. A. Hysterosalpingography findings in infertility - what has changed over the years? Afr. Health Sci. 19 (2), 1866–1874 (2019).
Nyengidiki, T. & Oriji, V. Comparative study of pain perception among infertile women undergoing Hysterosalpingography and Office Hysteroscopy in Port Harcourt, Nigeria. Clin. Obstet. Gynecol. Reprod. Med. 6(3), 1–5. (2020).
Kiykac Altinbas, S. et al. Evaluation of pain during hysterosalpingography with the use of balloon catheter vs metal cannula. J. Obstet. Gynaecol. 35 (2), 193–198 (2015).
Liu, X. et al. Diagnosis and treatment of fallopian tube obstruction: a literature review. Int. J. Clin. Exp. Med. 10 (12), 15950–15959 (2017).
O’Flynn, N. Assessment and treatment for people with fertility problems: NICE guideline. Br. J. Gen. Pract. 64 (618), 50–51 (2014).
Nia, S. S., Safi, F., Shoukrpour, M. & Kamali, A. An investigation into the effect of evening primrose in dilatation of cervix and pain during and after hysterosalpingography. J. Med. Life. 12 (3), 284 (2019).
Cicinelli, E. Hysteroscopy without anesthesia: review of recent literature. J. Minim. Invasive. Gynecol. 17 (6), 703–708 (2010).
Karaman, E., Çim, N., Alkış, İ., Yıldırım, A. & Yıldızhan, R. Rectal indomethacin use in pain relief during hysterosalpingography: a randomized placebo controlled trial. J. Obstet. Gynecol. Res. 42 (2), 195–201 (2016).
Tadesse, M. et al. Effect of preoperative anxiety on postoperative pain on patients undergoing elective surgery: prospective cohort study. Annals Med. Surg. 73, 103190 (2021).
Erkılınç, S. et al. The effect of a pre-procedure information video on anxiety levels in patients undergoing hysterosalpingography: a prospective case-control study. J. Turkish German Gynecol. Association. 19 (3), 137 (2018).
Chauhan, M. B., Lakra, P., Jyotsna, D., Nanda, S. & Malhotra, V. Pain relief during hysterosalpingography: role of intracervical block. Arch. Gynecol. Obstet. 287, 155–159 (2013).
Mollazadeh, S., Shahrahmani, N., Sadeghi, M. & Roudsari, R. L. The Impact of Group Counseling on Psychological Status of Iranian Infertile women: a systematic review. J. Midwifery Reproductive Health. 12(3), 42–78 (2024).
Boivin, J. A review of psychosocial interventions in infertility. Soc. Sci. Med. 57 (12), 2325–2341 (2003).
Frederiksen, Y., Farver-Vestergaard, I., Skovgård, N. G., Ingerslev, H. J. & Zachariae, R. Efficacy of psychosocial interventions for psychological and pregnancy outcomes in infertile women and men: a systematic review and meta-analysis. BMJ open. 5(1), e006592. (2015).
Gameiro, S. et al. ESHRE guideline: routine psychosocial care in infertility and medically assisted reproduction—a guide for fertility staff. Human reproduction. 1;30(11):2476-85. (2015).
Bal, S. & Kulakaç, Ö. Effect of comfort theory-based nursing care on pain and comfort in women undergoing hysterosalpingography: a randomized controlled trial. Revista Da Associação Médica Brasileira. 69, e20230798 (2023).
Begum, M. R. & Hossain, M. A. Validity and reliability of visual analogue scale (VAS) for pain measurement. J. Med. Case Rep. Reviews. 2(11), 2589–8647. (2019).
Rezvani, A. M. Correlation between visual analogue scale and short form of McGill questionnaire in patients with chronic low back pain. (2012).
Werner, F. et al. Limited temporal stability of the Spielberger State-Trait Inventory over 3.5 years. (2022).
Nikandish, R. et al. Translation and validation of the Amsterdam Preoperative Anxiety and Information Scale (APAIS) for Iranian population. Res. Med. 31 (1), 79–84 (2007).
Daniali, S. S., Shahnazi, H., Kazemi, S. & Marzbani, E. The effect of educational intervention on knowledge and self-efficacy for pain control in patients with multiple sclerosis. Materia socio-medica. 28 (4), 283 (2016).
Wittenborn, J. et al. Anxiety in women referred for colposcopy: a prospective observational study. Arch. Gynecol. Obstet. 1–6 (2022).
Guvenc, G., Bektas Pardes, B., Kinci, M. F. & Karasahin, K. E. Effect of education and counselling on reducing pain and anxiety in women undergoing hysterosalpingography: a randomised controlled trial. J. Clin. Nurs. 29 (9–10), 1653–1661 (2020).
Lee, C-H. et al. Effects of educational intervention on state anxiety and pain in people undergoing spinal surgery: a randomized controlled trial. Pain Manage. Nurs. 19 (2), 163–171 (2018).
Hsueh, F-C. et al. A study on the effects of a health education intervention on anxiety and pain during colonoscopy procedures. J. Nurs. Res. 24 (2), 181–189 (2016).
ISBN: 978-1-4419-1004-2 Hollie B. Hospital Anxiety.Encyclopedia of Behavioral Medicine & Pellosmaa Tamer F. Desou (2013).
Sezer, N. Y., Aker, M. N., Gönenç, İ. M., Topuz, Ş. & Şükür, Y. E. The effect of virtual reality on women’s perceived pain, fear, anxiety, and views about the procedure during hysterosalpingography: a randomized controlled trial. Eur. J. Obstet. Gynecol. Reproductive Biology. 286, 5–9 (2023).
Balci, O., Acar, A., Mahmoud, A. S. & Colakoglu, M. C. Effect of pre-amniocentesis counseling on maternal pain and anxiety. J. Obstet. Gynecol. Res. 37 (12), 1828–1832 (2011).
Sabourimoghaddam, H. et al. Effect of stressful stimulus on blood pressure and heart rate in patients with cardiorascular disease in comparison with healthy subjects based on emotion seeking levels. J. Mod. Psychol. Researches. 10 (38), 149–165 (2015).
Babaei-Sis, M. et al. The effect of educational intervention of life style modification on blood pressure control in patients with hypertension. J. Educ. Community Health. 3 (1), 12–19 (2016).
Acknowledgements
This study was carried out with the kind collaboration of the participants.
Funding
None.
Author information
Authors and Affiliations
Contributions
SZ.H, F. A, and Sh.JS contributed to the conception and design of the study; F. A, Sh.JS, and SZ.H did the literature search; SH.JS, SZ.H, and F. A performed the statistical analysis; Z. D, F. AH, Sh.JS, F.A, and SZ.H, A.O wrote the first draft of the manuscript. All authors contributed to the manuscript revision and read and approved the submitted version.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
The study protocol was approved by the Ethics Committee of Tarbiat Modares university (code: IR.MODARES.REC.1401.144). All procedures were in accordance with the ethical standards of the Regional Research Committee and with the Declaration of Helsinki 1964 and its later amendments. After explaining the study’s purposes, informed written consent and verbal assent were obtained from all participants. They were informed that their participation was voluntary, confidential and anonymous, and that they had the right to withdraw from the research at any time.
Consent for publication
Not applicable.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Daneshfar, Z., Sadatmahalleh, S.J., Hosseini, S.Z. et al. A randomized controlled trial on the impact of a specialized training program on anxiety and perceived pain in infertile women undergoing hysterosalpingography. Sci Rep 14, 26396 (2024). https://doi.org/10.1038/s41598-024-76881-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-76881-1
