
Abstract
Muscle weakness is a risk factor for multiple diseases. However, most protocols to assess muscle weakness require clinical settings. A difficulty lifting 5 kg may be a simple measure of muscle weakness in domestic settings. However, no relevant study on assessing muscle weakness has been reported. We investigated the associations of difficulty lifting 5 kg with various musculoskeletal, cardiovascular, metabolic, and neurological diseases in geriatric adults aged 50 or above from 15 countries (n = 51,536) over five years. The data was collected by the Survey of Health, Ageing, and Retirement in Europe (SHARE) conducted between 2013 and 2020. Overall, 10,025 (19.5%) respondents exhibited difficulty lifting 5 kg at baseline in 2013. Over the next four years, these respondents exhibited higher risks for developing a low quality of life (QoL) (9.42%), depression (8.14%), low handgrip strength (7.38%), and osteoarthritis (6.98%) after adjusting for age and gender. Additionally, these respondents exhibited mild to moderate risks for developing rheumatoid arthritis, heart attack, diabetes mellitus, hypertension, Alzheimer’s disease, stroke, or hip fracture (all p < 0.05). After adjusting for age and country, the risks of developing various diseases were higher in men than in women. Collectively, difficulty lifting 5 kg can herald the onset of several cardiovascular, neurological, and musculoskeletal disorders along with a reduced QoL. We suggest that difficulty lifting 5 kg may be a valuable indicator of muscle weakness and poor health in domestic settings.
Similar content being viewed by others

Introduction
Physiological aging is associated with a progressive loss of muscle strength in both genders1. It is generally recognized that muscle weakness in these patients is associated with an increased risk of several age-related diseases2. Muscle weakness in old age exhibits significant prognostic potential for cardiovascular, nervous, gastrointestinal, renal, skeletal, and respiratory diseases3. Consequently, muscle weakness increases the risk of hospitalization, functional disability, and mortality. A bidirectional interface is proposed so muscle weakness increases disease severity and vice versa4. Thus, a timely identification of individuals with muscle weakness may be imperative to improve desirable patient outcomes.
In most diseases, muscle weakness may precede muscle atrophy, establishing its efficacy in predicting and monitoring disease outcomes5. In addition, muscle weakness appears superior to muscle wasting in predicting survival and disability in older adults6. Due to its prognostic potential, muscle weakness is considered a preliminary sign of sarcopenia or age-related muscle decline by the European Working Group on Sarcopenia in Older People (EWGSOP2)7. Handgrip strength (HGS) measurement is a simple test to investigate muscle weakness. The measurement involves squeezing a hand-held dynamometer with the maximal possible strength. A low HGS may help predict several age-related diseases, such as cancer, stroke, metabolic disorders, osteoporosis, and cardiac failure8.
Normative values for HGS are described for various countries9. However, significant differences exist in the HGS values across regions. For example, the average HGS values for men aged 61–70 are 42 kg among Europeans but only 27 kg among South Asians9. The variations in socioeconomic status, ethnicities, dietary patterns, and lifestyles may partly account for these differences in HGS. In addition, the instruments for measuring HGS may vary across countries. Most relevant studies involve four types of HGS dynamometers, including hydraulic, pneumostatic, spring-type, and strain hand dynamometers10. However, the comparative studies report inconsistencies among their readings, questioning the reliability and validity of these dynamometers10,11. In addition, variable prices, limited access to purchase channels, and constant maintenance and calibration may hinder the suitability of these dynamometers for domestic usage.
Thus, it may be imperative to perform a simple and preliminary evaluation of muscle strength before standardized testing, including HGS measurements and laboratory investigations. An ability to lift 5 kg of weight may be a simple and transparent measure of muscle strength in most domestic and clinical settings. This test is inexpensive and can be performed with multiple household objects. It is plausible that this test may be associated with muscle weakness and various age-associated diseases similar to HGS measurement. However, such an investigation has never been reported before.
This study aimed to evaluate the associations of muscle weakness, as determined by difficulty lifting 5 kg of weight, with the future development of various health conditions. The 5-kg threshold was selected due to its relevance to everyday household objects, such as a standard bag of sugar or all-purpose flour, an average house cat, an air fryer, a portable slow cooker, and the cast iron Dutch oven. Thus, the study provides a practical and accessible measure of muscle strength and overall health within the domestic environment. We used a longitudinal cohort study design to investigate the prognostic value of self-reported difficulty lifting 5 kg of weight for several age-related diseases and quality of life (QoL) among older adults from 15 countries.
This study used the standardized Survey of Health, Ageing, and Retirement in Europe (SHARE) dataset12. Participants aged 50 and older were recruited due to their relevance to age-related disorders. Fifteen geographically proximate countries with relatively homogenous racial, cultural, and ethnic profiles were selected for inclusion. This selection was further supported by our prior research indicating a similar prevalence of muscle weakness among older adults in these countries13. We hypothesized that difficulty lifting 5 kg of weight will be associated with a significantly higher risk of developing several age-related degenerative, metabolic, and proliferative diseases in an age- and gender-specific manner in the geriatric population of 15 countries from Europe and the Middle East.
Materials and methods
The SHARE dataset comprises a harmonized longitudinal panel survey conducted on individuals aged 50 years and older across multiple European countries and Israel14. Data collection occurred through computer-assisted personal interviews (CAPI), covering various domains, such as demographic characteristics, socioeconomic indicators, living conditions, and physical and mental health. For this analysis, the baseline dataset utilized was derived from the fifth wave of SHARE conducted in 2013. Follow-up information on the participants’ health was provided in subsequent SHARE waves (6, 7, and 8) conducted in 2015, 2017, and 2019/2020, respectively, as described on the SHARE website15. The sample encompasses 15 countries: Austria, Germany, Sweden, Netherlands, Spain, Italy, France, Denmark, Switzerland, Belgium, Israel, Czech Republic, Luxembourg, Slovenia, and Estonia.
The experimental protocols described in this study were approved by the ethics board of Max-Planck-Society (Germany). Information and documentation on the ethics approval is available on the SHARE website (see FAQ Sect. 3.11 https://share-eric.eu/data/faqs-support. All experiments were carried out in accordance with relevant guidelines and regulations. A written informed consent was obtained from all study participants.
The detailed exclusion criteria are previously described14. Briefly, individuals were excluded if they were incarcerated, hospitalized, or out of the country for the entire survey period, unable to speak the country’s language(s), or had moved to an unknown address. All SHARE respondents previously interviewed in the longitudinal study were traced and re-interviewed if they moved within the country14.
Respondents were asked to report if they had any difficulty doing various everyday activities. Difficulties that were expected to last less than three months at the time of responses were excluded. One of the activities was “lifting or carrying weights over 5 kilos”, which is the central indicator in this analysis. Difficulties in lifting 5 kg, age (10 years intervals), gender, and country of residence were the baseline information obtained from wave 5.
The evaluation of HGS was conducted utilizing a hand-held dynamometer. Participants were directed to press the dynamometer using their left and right hands, with each repetition performed twice. The highest recorded value from the four measurements were utilized for subsequent analysis. Low HGS was categorized according to gender-specific thresholds as defined by the guidelines established by the EWGSOP2, with a threshold of 27 kg for men and 16 kg for women7.
The quality of life (QoL) was assessed using the CASP-12 index, which covers four dimensions (Control, Autonomy, Self-realization, and Pleasure), each with 3 questions12. The sample questions are: (1) How often do you think your age prevents you from doing the things you would like to do? (2) How often do you think that shortage of money stops you from doing the things you want to do? (3) How often do you feel that the future looks good for you? Participants were instructed to assess the frequency of specific feelings or thoughts using response categories “often,” “sometimes,” “rarely,” or “never.” Based on numerical scores of 1 (often) to 4 (never), the CASP-12 index was generated by the sum of the scores from the 12 indicators. Consequently, the index ranged from 12 (indicating minimum well-being) to 48 (maximum well-being). For the present study, an indicator for low well-being was generated, defined by scores less than or equal to 29.
Depressive symptoms were assessed utilizing the Euro-D depression scale16. Euro-D is an additive index based on the number of reported depressive symptoms. A total of 12 symptoms were asked, including sadness, having no hopes for the future, sleep disturbances, feelings of guilt, irritability, and loss of appetite. The Euro-D scale scores ranged from 0 to 12, with higher scores indicating more significant depressive symptoms. For the present study, an indicator for high depression level was generated, defined by scores greater than or equal to 6.
All other medical conditions were collected through a list of diseases presented to the respondents, who indicated whether they had these conditions or if they had received a doctor’s diagnosis: heart attack (including myocardial infarction or coronary thrombosis or any other heart problem including congestive heart failure); chronic lung diseases; hip fracture; rheumatoid arthritis; high blood pressure or hypertension; high blood cholesterol; diabetes or high blood sugar; cancer or malignant tumours (including leukaemia or lymphoma, but excluding minor skin cancers); Alzheimer’s disease, dementia, organic brain syndrome, senility or any other serious memory impairment; stroke or cerebral vascular disease; osteoarthritis or other rheumatism.
The gross sample size was 51,536, with demographic details about gender and age. However, we found missing information about various diseases and conditions, either because the respondent could not answer, or did not want to answer, or simply did not know the answer. The number of missing observations varied for various diseases and ranged from 687 (Alzheimer’s disease) to 20,557 (high blood pressure). The respondents with missing information were excluded in relevant analysis as is evident by the varying displayed sample sizes for individual diseases or conditions in Table 1.
Statistical analysis
Multiple regression analyses were employed to identify the associations of the difficulty of lifting 5 kg on the risk of future medical conditions. To ease the interpretation of estimated parameters, we apply a linear probability model17 with robust standard errors, as described by the following regression equation:
Here, π represents the risk of a medical condition, for example, high blood pressure. The variables \(X_{1} , X_{2} , \ldots ,X_{k}\) represent baseline characteristics (gender, age, and difficulties lifting 5 kg, etc.) influencing the medical condition, while \(\beta_{1} ,\beta_{2} , \ldots ,\beta_{k}\) denote the corresponding effects. The symbol \(\epsilon\) accounts for the error term. Estimated parameters are presented as percentage points change (fraction) in the risk of a given condition. The relative risk ratio (RRR) was measured as RRR = (estimate + average risk) / (average risk) = \({\raise0.7ex\hbox{${\left( {\hat{\beta } + \overline{\pi }} \right)}$} \!\mathord{\left/ {\vphantom {{\left( {\hat{\beta } + \overline{\pi }} \right)} {\overline{\pi }}}}\right.\kern-0pt} \!\lower0.7ex\hbox{${\overline{\pi }}$}}\). An alternative is to use the probit or logit models, but their estimated parameters are not easily interpretable without a transformation into probabilities. Statistical analyses were performed using STATA software package version 18.0 (StataCorp LLC, College Station, TX).
Results
The essential characteristics of the study population are described in Table 1. Information on gender, age, and lifting 5 kg was obtained from the baseline year 2013. A total of 51,536 respondents were included in the study, of which 41,511 (80.5%) respondents had no difficulty lifting 5 kg at the baseline year in 2013, while 10,025 (19.5%) respondents exhibited difficulty lifting 5 kg. Women represented 56.1% of the study population. The youngest age group, aged 50–59 years, represented 11.3%, while the oldest age group, 90 or above, represented 4% of the study population (Table 1). For a given disease, we excluded the participants who already had the disease at the baseline year of 2013. Thus, the sample sizes varied for various diseases. For example, 30,979 out of the 51,536 participants did not suffer from high blood pressure in 2013. However, 21.5% of respondents developed high blood pressure between 2014 and 2020. Among those with difficulty lifting 5 kg in 2013, 26.2% of participants developed high blood pressure in the subsequent years. Conversely, among those with no difficulty lifting 5 kg in 2013, 20.6% of the respondents developed high blood pressure in subsequent years (Table 1). Further, 49,864 respondents had no hip fracture in 2013. However, 1.8% of them developed hip fractures during subsequent years. Among those with difficulty lifting 5 kg, 3.5% of respondents developed hip fractures. Conversely, among those with no difficulty lifting 5 kg, 1.5% of respondents developed hip fractures in subsequent years (Table 1).
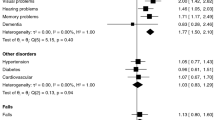
Figure 1 represents the estimated higher risks for developing a given disease in 2014–2020 for the respondents with difficulty lifting 5 kg in 2013 after controlling for gender, age, and country of residence. The most significant effect was observed for developing a low QoL, where the risk increased by 9.42% points (95% C.I = 8.47–10.37% points). We also observed significant increased risks of developing depression (8.14% points, 95% CI = 7.05–9.23%), low HGS (7.38% points, 95% CI = 6.52–8.24%), and osteoarthritis (6.98% points, 95% CI = 5.93–8.03%) (Fig. 1). Conversely, the increased risk of developing stroke (1.78% points, 95% CI = 1.27–2.29%) and hip fracture (1.16% points, 95% CI = 0.77–1.55%) were low among respondents with difficulty lifting 5 kg (Fig. 1).

Regression coefficients and 95% confidence intervals from all respondents with difficulty lifting 5-kg on the incidence of various musculoskeletal, metabolic, cardiovascular, and neurological diseases. The CI for cancer has been truncated from a slightly negative value to 0.
We next investigated the risks of developing given diseases among participants with difficulty lifting 5 kg in the baseline year, based on age and gender (Tables 2–5). We divided the men and women into two age groups, including 50–65 years and 66 and above. Among men aged 50–65, difficulty lifting 5 kg was associated with a significantly higher risk of developing all investigated diseases except cancer (Table 2). The highest relative risk ratio (RRR) was observed for developing depression (RRR = 3.42) among respondents with difficulty lifting 5 kg. We also observed significantly higher risks for developing low QoL (RRR = 3.16), low HGS (RRR = 2.69), and Alzheimer’s disease (RRR = 2.59) (Table 2).
Among women aged 50–65, difficulty lifting 5 kg was associated with significantly higher risks of developing all diseases except cancer and hip fracture (Table 3). The highest RRR was obtained for a low HGS (RRR = 2.81), followed by poor QoL (RRR = 2.28), Alzheimer’s disease (RRR = 2.06), and high depression (RRR = 2.03) (Table 3). Similarly, among men aged 66 or above, difficulty lifting 5 kg increased the risk of developing all investigated diseases except cancer and heart attack. The highest RRR was observed for developing a poor QoL (RRR = 2.49), followed by high depression (RRR = 2.25) and low HGS (RRR = 2.18) (Table 4). Next, among women aged 66 or above, difficulty lifting 5 kg increased the risk of all diseases except cancer and high blood pressure. The highest RRR was observed for poor QoL (RRR = 1.81), followed by low HGS (RRR = 1.76) and high depression (RRR = 1.65) (Table 5).
Lastly, we presented an average disease effect based on all the diseases investigated in this study. We found that the risk of developing diseases was higher in men than women for a given age group. For example, among the respondents aged 50–65, RRR for the average disease effect was 2.09 in men (Table 2) and 1.8 in women (Table 3). Similarly, for the respondents aged 66 or above, the RRR for the average disease effect was 1.57 for men (Table 4) and 1.41 for women (Table 5).
Discussion
In this large-scale study of 51,536 geriatric adults from 14 European countries and Israel, we report significant associations of a self-reported difficulty to lift 5 kg of weight with several chronic diseases and reduced QoL. Specifically, difficulty in lifting 5 kg of weight was associated with increased risks of a deficient QoL, higher scores on the Euro depression scale, chronic lung diseases, hip fracture, rheumatoid arthritis, high blood cholesterol, Alzheimer’s disease, stroke, and osteoarthritis irrespective of age and gender. Conversely, similar associations were not found between difficulty lifting 5 kg of weight and the risk of diabetes mellitus or cancer.
We observed an elevated risk of developing low HGS among participants with difficulty lifting 5 kg in both age groups and genders. This observation is consistent with the fact that lifting 5 kg of weight primarily requires the contraction of handgrip muscles. We used the cut-off values of 27 kg for men and 16 kg for women as defined by the EWGSOP27. Conversely, the weight of 5 kg was used for both genders. Despite this discrepancy, the risk of developing low HGS was similar between genders aged 50–65. On the other hand, men aged 66 or above exhibited a higher risk of developing low HGS than women of the same age with difficulty lifting 5 kg of weight. Men have stronger muscles than women due to anabolic hormones. Thus, difficulty in lifting a similar weight indicates significantly more muscle weakness in men than in women, which is consistent with our observation among participants aged 66 or above. Interestingly, we also observed that the coupling between the difficulty in lifting 5 kg of weight and the risk of developing low HGS was stronger after 65 years of age. This finding is consistent with age-related muscle degeneration, which reflects the loss of muscle mass and strength.
Several mechanisms explain the association between difficulty lifting 5 kg of weight and the diseases investigated in this study. First, muscle weakness in these participants suggests a sedentary lifestyle and low physical activity18, which are risk factors for several diseases reported here19. For example, a sedentary lifestyle is associated with higher risks of depression, cardiovascular diseases, metabolic disorders, and neurological deficits. It is also known that muscle weakness and low levels of physical fitness track in childhood and/or adolescence into advanced age20. Second, a significant coupling exists between muscle strength and mass. Thus, participants with difficulty lifting 5 kg will likely exhibit muscle wasting. Muscle mass is a significant protein reserve that protects against organ degeneration due to trauma, diseases, and/or aging21. Thus, a low muscle mass in the participants with difficulty lifting 5 kg of weight can predispose them to develop chronic diseases. Third, significant associations of muscle weakness are reported with systemic inflammation. It is also established that chronic low-grade inflammation can cause and/or exacerbate various cardiovascular, neurological, and metabolic disorders reported in this study. Fourth, a causal interface is described between muscle weakness and oxidative stress22. Thus, individuals with muscle weakness may have elevated oxidative stress and vice versa. It is generally recognized that oxidative stress contributes to several systemic diseases23. Thus, difficulty lifting 5 kg of weight may increase the risk of developing chronic diseases.
Among various conditions, a low QoL and higher scores on the Euro depression scale exhibited the most robust associations with difficulty in lifting 5 kg of weight. The association between muscle weakness and poor QoL is well-recognized24. We have also previously reported reduced QoL in older adults with reduced HGS25. We used the CASP-12 survey here, an internationally standardized tool to measure QoL. A positive association between HGS and CASP-12 has been reported in both genders26, which is consistent with our observation of poor QoL in patients with difficulty lifting 5 kg of weight. The association between poor QoL and muscle weakness is probably attributed to a dependence on the activities of daily living in these patients due to muscle weakness. CASP-12 investigates autonomy, control, pleasure, and self-realization, which are partly dependent on functional and healthy muscles.
A negative correlation between HGS and depression is well established27. Thus, the patients with reduced HGS exhibit a higher prevalence of depression and vice versa27. Consistent with these findings, we observed a higher risk of depression in participants with difficulty lifting 5 kg of weight. These participants also exhibited cognitive impairment, as evidenced by a higher risk of developing Alzheimer’s disease (AD). This observation agrees with our previous reports of associations between low HGS and AD in older adults28. The potential mechanisms associating difficulty in lifting 5 kg of weight with depression and AD may involve altered body biochemistry and lifestyle changes27. Muscle strength is negatively influenced by hormonal imbalance, systemic inflammation, and oxidative stress. These factors are also attributed to a higher risk of developing depression and AD27. In addition, the sedentary lifestyle in patients with muscle weakness can also increase the risks of acquiring depression and AD27.
The difficulty of lifting 5 kg of weight also emerged as a risk factor for rheumatoid arthritis (RA) and osteoarthritis. Both diseases share inflammation as a common pathophysiology with muscle weakness29. These participants had established muscle weakness before they developed joint diseases. Thus, muscle weakness and the difficulty in lifting 5 kg weight appear to precede RA and osteoarthritis and exhibit prognostic potential for these diseases. In addition, the association of the difficulty of lifting 5 kg with hip fracture supports the established coupling between muscle and bone health. However, it must be noted that RA, which primarily affects the small joints of the hands, may remain subclinical for a considerable time before an established clinical diagnosis is made. Thus, we cannot rule out that a subclinical RA may have contributed to the difficulty of lifting 5 kg of weight at baseline in the study participants.
Participants with difficulty lifting 5 kg weight also exhibited higher risks for developing several cardiovascular diseases, including high blood pressure, heart attack, high blood cholesterol, and stroke. This observation is supported by previous reports that associate low HGS with an elevated risk of morbidity and mortality due to cardiovascular diseases30.
Previous observations based on large population-based studies suggest inconsistent associations of HGS with cancer and cancer mortality3,31. Several factors may explain the disjunction between muscle weakness and cancer. We considered all types of cancers without consideration for individual cancer types. Previous studies suggest an association of muscle weakness with cancer in a cancer-specific manner. For example, a low HGS was associated with breast cancer in women and colorectal cancer in men31. However, the association between muscle weakness and cancer may be neutralized when all cancer types are pooled together. In addition, nutritional status and the use of specific gender-specific cut-offs for low HGS also affect the associations between muscle weakness and cancer risk31. We did not investigate the nutritional status of participants and considered a similar weight of 5 kg to evaluate muscle weakness in both genders, which may have influenced our observation. However, the HGS cut-off values for muscle weakness differ between men and women7. Thus, using different weights for men and women in this study may have been pertinent. Lastly, age-related muscle weakness may conceal cancer-related muscle weakness in advanced age31.
The major strength of this study is that it has a large representative sample from 14 European countries and Israel. The longitudinal design of the study enhances our confidence in the associations of muscle weakness with various diseases. All data was collected in a harmonized way across multiple European settings using the standardized SHARE questionnaire. However, this study has some limitations. The difficulty of lifting 5 kg of weight was self-reported. The normal HGS is lower in women than men7. However, we used 5 kg of weight as a tool to evaluate muscle weakness without discrimination for gender. We did not consider BMI and muscle mass while considering muscle weakness. Some participants may have subclinical illnesses during the assessment, which were overlooked in this study. A mild to moderate heterogeneity across various European countries may have partly affected our observations. Several participants had multiple comorbidities, which may affect our observations more than individual comorbidities’ cumulative effects. Lastly, the selective survival of the study participants may have influenced our data.
In conclusion, we report that a simple dysfunction, such as difficulty lifting 5 kg of weight, can herald the onset of several cardiovascular, neurological, and musculoskeletal disorders along with reduced QoL or mental health. We suggest that difficulty lifting a 5-kg weight may be used as an easy initial preliminary quick and transparent marker of muscle weakness before more sophisticated tools, such as an HGS dynamometer, are employed to assess muscle weakness. Our findings provide an effective, simple, inexpensive, and user-friendly assessment tool for muscle weakness in high-risk individuals in domestic and clinical settings.
Data availability
The data is publicly available after application from https://share-eric.eu/. The access to data requires individual free registration followed by the acceptance of the SHARE Conditions and signing the SHARE User Statement. After acceptance of these documents, data can be downloaded using the personal ID and password. This paper uses data from SHARE Waves 5, 6, 7, and 8 (DOIs: https://doi.org/10.6103/SHARE.w5.800, https://doi.org/10.6103/SHARE.w6.800, https://doi.org/10.6103/SHARE.w7.800, https://doi.org/10.6103/SHARE.w8.800). The SHARE data collection has been funded by the European Commission, DG RTD through FP5 (QLK6-CT-2001–00360), FP6 (SHARE-I3: RII-CT-2006–062193, COMPARE: CIT5-CT-2005–028857, SHARELIFE: CIT4-CT-2006–028812), FP7 (SHARE-PREP: GA N°211909, SHARE-LEAP: GA N°227822, SHARE M4: GA N°261982, DASISH: GA N°283646) and Horizon 2020 (SHARE-DEV3: GA N°676536, SHARE-COHESION: GA N°870628, SERISS: GA N°654221, SSHOC: GA N°823782, SHARE-COVID19: GA N°101015924) and by DG Employment, Social Affairs & Inclusion through VS 2015/0195, VS 2016/0135, VS 2018/0285, VS 2019/0332, and VS 2020/0313. Additional funding from the German Ministry of Education and Research, the Max Planck Society for the Advancement of Science, the U.S. National Institute on Aging (U01_AG09740-13S2, P01_AG005842, P01_AG08291, P30_AG12815, R21_AG025169, Y1-AG-4553-01, IAG_BSR06-11, OGHA_04-064, HHSN271201300071C, RAG052527A), and from various national funding sources is gratefully acknowledged (see www.share-project.org).
References
Karim, A. et al. Evaluation of sarcopenia using biomarkers of the neuromuscular junction in Parkinson’s disease. J. Mol. Neurosci. 72(4), 820–829 (2022).
Parvatiyar, M. S. & Qaisar, R. Editorial: Skeletal muscle in age-related diseases: From molecular pathogenesis to potential interventions. Front. Physiol. 13, 1056479 (2022).
Mey, R. et al. Handgrip strength in older adults with chronic diseases from 27 European countries and Israel. Eur. J. Clin. Nutr. 77(2), 212–217 (2023).
Soysal, P. et al. Handgrip strength and health outcomes: Umbrella review of systematic reviews with meta-analyses of observational studies. J. Sport Health Sci. 10(3), 290–295 (2021).
Mitchell, W. K. et al. Sarcopenia, dynapenia, and the impact of advancing age on human skeletal muscle size and strength; a quantitative review. Front. Physiol. 3, 260 (2012).
Cereda, E. et al. Muscle weakness as an additional criterion for grading sarcopenia-related prognosis in patients with cancer. Cancer Med. 11(2), 308–316 (2022).
Cruz-Jentoft, A. J. et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 48(4), 601 (2019).
Cheung, C. L. et al. Association of handgrip strength with chronic diseases and multimorbidity: A cross-sectional study. Age 35(3), 929–941 (2013).
Leong, D. P. et al. Reference ranges of handgrip strength from 125,462 healthy adults in 21 countries: A prospective urban rural epidemiologic (PURE) study. J. Cachexia Sarcopenia Muscle 7(5), 535–546 (2016).
Huang, L. et al. Reliability and validity of two hand dynamometers when used by community-dwelling adults aged over 50 years. BMC Geriatr. 22(1), 580 (2022).
Guerra, R. S. et al. Comparison of Jamar and bodygrip dynamometers for handgrip strength measurement. J. Strength Cond. Res. 31(7), 1931–1940 (2017).
Börsch-Supan, A. Survey of Health, Ageing and Retirement in Europe (SHARE) Wave 8. Release version: 8.0.0. SHARE-ERIC. Data set. (2022).
Qaisar, R. et al. Predictors of the onset of low handgrip strength in Europe: A longitudinal study of 42,183 older adults from 15 countries. Aging Clin. Exp. Res. 36(1), 162 (2024).
Borsch-Supan, A. et al. Data resource profile: The survey of health, ageing and retirement in Europe (SHARE). Int. J. Epidemiol. 42(4), 992–1001 (2013).
SHARE. Survey of Health, Ageing and Retirement in Europe (SHARE). 2025 [cited 2025 19th Feb 2025]; https://share-eric.eu/data/data-documentation/waves-overview.
Prince, M. J. et al. Development of the EURO-D scale–a European, Union initiative to compare symptoms of depression in 14 European centres. Br. J. Psychiatry 174, 330–338 (1999).
Wooldridge, J. M. A Binary Dependent Variable: The Linear Probability Model, in Introductory econometrics: A modern approach (Cengage, 2020).
Qaisar, R., Karim, A. & Elmoselhi, A. B. Muscle unloading: A comparison between spaceflight and ground-based models. Acta Physiol. 228(3), e13431 (2020).
Gonzalez, K., Fuentes, J. & Marquez, J. L. Physical inactivity, sedentary behavior and chronic diseases. Korean J. Fam. Med. 38(3), 111–115 (2017).
Garcia-Hermoso, A., Izquierdo, M. & Ramirez-Velez, R. Tracking of physical fitness levels from childhood and adolescence to adulthood: A systematic review and meta-analysis. Transl. Pediatr. 11(4), 474–486 (2022).
Buckner, S. L. et al. The association of handgrip strength and mortality: What does it tell us and what can we do with it?. Rejuvenation Res. 22(3), 230–234 (2019).
Powers, S. K., Smuder, A. J. & Judge, A. R. Oxidative stress and disuse muscle atrophy: Cause or consequence?. Curr. Opin. Clin. Nutr. Metab. Care 15(3), 240–245 (2012).
Forman, H. J. & Zhang, H. Targeting oxidative stress in disease: Promise and limitations of antioxidant therapy. Nat. Rev. Drug Discov. 20(9), 689–709 (2021).
Graham, C. D. et al. A systematic review of quality of life in adults with muscle disease. J. Neurol. 258(9), 1581–1592 (2011).
Qaisar, R. et al. A leaky gut contributes to reduced sarcopenia-related quality of life (SarQoL) in geriatric older adults. Qual. Life Res. 33(2), 551–559 (2024).
Marques, L. P. et al. Quality of life associated with handgrip strength and sarcopenia: EpiFloripa aging study. Arch. Gerontol. Geriatr. 81, 234–239 (2019).
Zasadzka, E. et al. Correlation between handgrip strength and depression in older adults—A systematic review and a meta-analysis. Int. J. Environ. Res. Public Health, 18(9) (2021).
Qaisar, R. et al. A leaky gut contributes to postural dysfunction in patients with Alzheimer’s disease. Heliyon 9(9), e19485 (2023).
Mohammed, A. et al. A comparison of risk factors for osteo- and rheumatoid arthritis using NHANES data. Prev. Med. Rep. 20, 101242 (2020).
Liu, W. et al. The association of grip strength with cardiovascular diseases and all-cause mortality in people with hypertension: Findings from the prospective urban rural epidemiology China study. J. Sport Health Sci. 10(6), 629–636 (2021).
Zhuang, C. L. et al. Associations of low handgrip strength with cancer mortality: A multicentre observational study. J. Cachexia Sarcopenia Muscle 11(6), 1476–1486 (2020).
Acknowledgements
The authors extend their appreciation to the Researchers Supporting Project number (RSP2025R277), King Saud University, Riyadh, Saudi Arabia for funding the current study. The authors also extend their appreciation to a grant from the German Federal Ministry of Education and Research (BMBF) as part of SHARE (grant numbers: 01UW1801/01UW2202).
Funding
The authors extend their appreciation to the Researchers Supporting Program at King Saud University in Saudi Arabia for funding this research work through the project no. (RSP#2025R277). This work is supported by a grant from the German Federal Ministry of Education and Research (BMBF) as part of SHARE (grant numbers: 01UW1801/01UW2202).
Author information
Authors and Affiliations
Contributions
Conceptualization; R.Q, M.H, A.K, F.A, F.F, A.A, M.A. & S.A. Data curation; M.H & F.F. Formal analysis; M.H & F.F, Funding acquisition; M.A. & S.A. Investigation; R.Q, M.H, A.K, F.A, F.F, A.A, & S.A. Methodology; M.H & F.F. Project administration; R.Q, M.H, A.K, F.A, F.F, A.A, M.A & S.A. Resources; R.Q, M.H, A.K, F.A, F.F, A.A, M.A & S.A. Supervision; R.Q, M.H, A.K, F.A, F.F, A.A, & S.A. Validation; M.H, & F.F, Writing—original draft; R.Q, M.H, A.K, F.A, F.F, A.A, M.A & S.A. Writing—review & editing; R.Q, M.H, A.K, F.A, F.F, A.A, M.A & S.A.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Qaisar, R., Hussain, M.A., Franzese, F. et al. The simple task of lifting five kilograms serves as a predictor of age-related disorders in old adults. Sci Rep 15, 17833 (2025). https://doi.org/10.1038/s41598-025-03128-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-025-03128-y
