
Abstract
This retrospective observational multicentre cohort study compared the rate of postoperative cystoid macular oedema (CME) between two intraocular lens (IOL) scleral fixation (SFIOL) techniques: a flanged IOL fixation technique (Yamane technique) and a suture IOL transscleral fixation technique (conventional technique). The study included 207 eyes with postoperative CME that had undergone SFIOL and were observed for > 12 weeks between January 2019 and January 2021. The primary endpoint was a comparison of the rate of postoperative CME at 3 months between groups. Secondary endpoints were a comparison of postoperative best-corrected visual acuity (BCVA) at 3 months between groups and an analysis of characteristics associated with postoperative CME in the Yamane technique group. The Yamane technique group developed postoperative CME in 13.0% of eyes at 3 months, compared with 1.9% in the conventional technique group (odds ratio: 7.99, P = 0.045). Postoperative BCVA was consistently significantly higher in the Yamane technique group. Although many retinal surgeons have performed the Yamane technique because of its convenience for SFIOL, our findings suggest that the Yamane technique carries an increased risk of postoperative CME compared with the conventional suture method. Therefore, careful management of postoperative CME is needed after SFIOL.
Similar content being viewed by others


Introduction
For secondary intraocular lens (IOL) implantation, four techniques are available: IOL placement in the capsular bag, IOL in the ciliary sulcus, iris-fixated IOL, and scleral-fixated IOL (SFIOL). The first two options require an intact anterior capsule, and iris fixation requires sufficient iris tissue. If these conditions are not met, SFIOL is the only viable option.
In 2014, Dr. Yamane and colleagues reported sutureless 27-gauge needle-guided intrascleral IOL implantation (double-needle technique, also known as the Yamane technique), which eliminated the need for scleral dissection and suturing1,2. Since then, the Yamane technique has rapidly expanded worldwide because the technique is more convenient than conventional suture IOL transscleral fixation (conventional technique), which requires complex suturing to secure the IOL3. Furthermore, many retinal surgeons have attempted to develop a similar SFIOL method4,5,6,7,8,9,10,11,12,13,14,15,16,17. Although we have used the Yamane technique in many cases, our experience suggests that the rate of postoperative cystoid macular oedema (CME) is increasing. Moreover, some studies have shown that postoperative CME is significantly more common in patients who undergo the Yamane technique than in those who undergo conventional techniques18,19.
CME is characterised by macular thickening; risk factors include diabetes, uveitis, retinitis pigmentosa, retinal vein occlusion, the use of E2-prostaglandins, and eye surgeries. Although the Yamane technique is technically more convenient than conventional SFIOL and theoretically should cause less surgery-related inflammation, our experience and the existing literature suggest that it actually leads to a higher incidence of postoperative CME. This increased incidence could be caused by chronic inflammation due to subclinical pseudophacodonesis and iris chafing. Therefore, we hypothesised that the inflammation associated with the Yamane technique is more severe than that observed with conventional methods, resulting in a higher rate of postoperative CME.
Here, we retrospectively examined cases in which patients underwent SFIOL to compare the Yamane and conventional techniques; our analysis was conducted in eight institutions within the Japan Clinical REtina STudy group (J-CREST). Additionally, we examined potential predictive factors for postoperative CME in eyes that underwent SFIOL using the Yamane technique.
Methods
Study design and eligibility
This multicentre, retrospective study included 207 eyes that had undergone SFIOL using the Yamane or conventional techniques in eight J-CREST institutions (Hyogo Medical University, Kagoshima University Graduate School of Medical and Dental Sciences, Shiga University of Medical Science, St. Marianna University School of Medicine, Tokushima University Graduate School, University of Fukui, Mie University, and Kurume University School of Medicine) between January 2019 and January 2021. Data were extracted from medical records in participating hospitals and sent to the data centre in the Department of Ophthalmology, Hyogo Medical University. Clinical data were collected at each hospital through chart reviews or contact with patients or relatives. This study was performed in accordance with the Declaration of Helsinki, and the study protocol was approved by the ethics committees of Hyogo Medical University (approval no. 3559). The requirement for written informed consent from each patient was waived by the ethics committees because the study used clinical information that was obtained during routine clinical practice. Patients and the public were not involved in the design, conduct, reporting, or dissemination plans for this study.
Patients
Medical records were collected for patients who had undergone SFIOL using the Yamane technique or conventional technique. The postoperative follow-up period was > 12 weeks for all included patients. There was no age limit. If surgery was performed on both eyes in the same patient, only data for the right eye were included in the study. We also excluded eyes with epiretinal membrane and/or CME at the initial visit, as well as patients with diabetes mellitus. In total, 207 eyes from 207 patients were included (see Supplementary Figure S1 online). All clinical data are available online (see Supplementary Table S1). In a previous report on 65 eyes that underwent SFIOL, postoperative CME occurred in seven eyes (11%) that underwent the Yamane technique20. In our current study, we analysed 207 IOLs and hypothesised that CME, the primary endpoint, would occur in 23 eyes. In this observational study, we considered factors such as age, preoperative BCVA, and duration of surgery as potential contributors to the outcome. We anticipated that the multivariate logistic model would remain stable after adjusting for two or three of these confounding factors.
Surgical procedure
All patients underwent full vitrectomy using a 27-gauge system. The Yamane technique was performed as previously reported1,2. The conventional technique was performed using sutures; the two suture points involved scleral tunnels, as previously reported3.
Study protocol
The following patient characteristics were analysed: age, sex, involved eye, duration of surgery, preoperative lens condition (subluxated, IOL dislocation, or aphakia), time since previous cataract surgery, reason for SFIOL (pseudoexfoliation syndrome, acute angle-closure glaucoma, trauma, high myopia, atopy, artificial aphakia, complications during cataract surgery, unknown, and other), best-corrected visual acuity (BCVA; preoperatively and at 4 and 12 weeks postoperatively), number of corneal endothelial cells, flare grade (determined by laser flare meter; FM-600α, Kowa, Tokyo, Japan), and surgery-related complications, including postoperative CME. CME was diagnosed on the basis of optical coherence tomography-detected cystoid space in the fovea. Decimal visual acuity was determined using a Landolt chart at a distance of 5 m, with chart illuminance of 500–1000 lx. BCVA was measured on a Japanese Snellen chart, and Snellen values were converted to logarithm of the minimum angle of resolution (logMAR). For “off-chart” visual acuity values, such as counting fingers, hand motion, and light perception, logMAR values were regarded as 2.0, 2.3, and 2.6, respectively21.
Patients were followed up for > 12 weeks after surgery. Ophthalmic examinations were performed at 4 and 12 weeks postoperatively. For analysis, patients were placed into Yamane technique and conventional technique groups.
Study endpoints
The primary endpoint was a comparison of the rate of postoperative CME at 3 months between the Yamane technique and conventional technique groups. Secondary endpoints were a comparison of postoperative BCVA at 3 months between groups, and an analysis of characteristics associated with postoperative CME in patients who underwent SFIOL using the Yamane technique. Another endpoint comprised the identification of predictive factors for postoperative CME among patients in the Yamane technique group. Additionally, baseline characteristics were determined for all patients.
Statistical analyses
Categorical variables (presented as numbers and percentages) were compared using the χ2 test or Fisher’s exact test. Continuous variables (presented as either mean and standard deviation or median and interquartile range) were compared using Student’s t-test or the Wilcoxon rank-sum test.
Adjusted odds ratios for all endpoints were determined by comparison between the Yamane technique and the conventional technique using a logistic regression model adjusted for age, preoperative BCVA, and surgical duration.
Statistical analyses were performed using JMP® Pro (version 14.0.0, SAS Institute Inc., Cary, NC, USA). For all analyses, p-values were reported, along with two-sided 95% confidence intervals for point estimates. Statistical significance was regarded as P < 0.05.
Results
Baseline characteristics
For the 207 eyes included in this study, baseline characteristics are shown in Table 1. Patient age (mean ± standard deviation) was 66.4 ± 17.3 years, and patients were predominantly men (135 patients, 65.2%). Patients were separated into the following two groups: Yamane technique (155 eyes) and conventional technique (52 eyes). Preoperative lens conditions were subluxated lens (48 eyes, 23.2%), IOL dislocation (119 eyes, 57.5%), and aphakia (40 eyes, 19.3%). The top three causative diseases were unknown (75 eyes, 36.2%), pseudoexfoliation (33 eyes, 15.9%), and complications during cataract surgery (31 eyes, 15.0%). There were significant differences in age, sex, duration of surgery, causative disease, and preoperative BCVA between the two groups. The mean time since previous cataract surgery was 116 [48–192] months (i.e., ~ 16 years).
Primary endpoint: rate of postoperative CME at 3 months
Postoperative data are shown in Table 2. Postoperative CME was observed in 7.3% of eyes at 1 month and 10.6% of eyes at 3 months. The Yamane technique group developed postoperative CME in 13.0% of eyes at 3 months, compared with 1.9% in the conventional technique group (odds ratio: 7.99, 95% confidence interval [1.05–60.97], P = 0.045) (Table 3).
Secondary endpoint: postoperative BCVA at 3 months
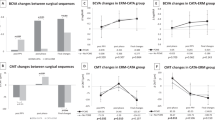
Postoperative BCVA was significantly higher in the Yamane technique group (0.1 logMAR at 1 month, 0.046 logMAR at 3 months) than in the conventional technique group (0 logMAR at 1 month, 0 logMAR at 3 months) throughout the follow-up period (Table 2). However, there was no significant difference in the rate of postoperative BCVA below 1.0 logMAR at 3 months between the Yamane technique and conventional technique groups (Table 3).
Predictive factors for postoperative CME in eyes that underwent SFIOL using the Yamane technique
Univariate and multivariate analyses were performed to identify the relationships of 12 factors with postoperative CME in eyes that underwent SFIOL using the Yamane technique: age, sex, involved eye, duration of surgery, preoperative lens condition, causative disease, preoperative BCVA, preoperative anterior inflammation, preoperative number of corneal endothelial cells, absence of postoperative transient ocular hypotension, absence of postoperative IOL capture, and absence of postoperative vitreous haemorrhage (Table 4).
Univariate analysis showed that longer duration of surgery (P = 0.0003), higher rate of pseudoexfoliation (P = 0.0006), lower preoperative number of corneal endothelial cells (P = 0.04), and absence of postoperative transient ocular hypotension (P = 0.0009) were factors significantly associated with postoperative CME at 3 months (Table 4).
Multivariate analysis of these factors revealed that all four factors were significantly associated with postoperative CME at 3 months: longer duration of surgery (P = 0.01), higher rate of pseudoexfoliation (P < 0.0001), lower preoperative number of corneal endothelial cells (P = 0.04), and absence of postoperative transient ocular hypotension (P = 0.0002) (Table 4).
Discussion
Since the Yamane technique was developed, its convenience has led to rapid expansion worldwide1,2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17. Subsequently, many ophthalmologists attempted to develop superior techniques for SFIOL. However, few clinicians have considered the limitations of these techniques18,19,20. The present analysis was conducted to examine the benefits and limitations of the Yamane technique.
Regarding the primary endpoint, postoperative CME was detected at a significantly higher rate in eyes that underwent SFIOL using the Yamane technique compared with eyes that underwent SFIOL using the conventional technique; this difference persisted at all follow-up time points. This finding was consistent with postoperative BCVA results, which were worse in the Yamane technique group than in the conventional technique group. However, our findings regarding the rate of postoperative BCVA below 1.0 logMAR at 3 months suggest that the rate of legal blindness (i.e., BCVA below 1.0 logMAR) does not significantly differ between the Yamane technique and the conventional technique. The Yamane technique is convenient because of its shorter surgical duration, but it can lead to a higher rate of postoperative CME, thereby impacting BCVA improvement.
Additionally, we performed univariate and multivariate analyses to identify potential predictive factors for postoperative CME. Both analyses showed that four factors (longer duration of surgery, higher rate of pseudoexfoliation, lower preoperative number of corneal endothelial cells, and absence of postoperative transient ocular hypotension) were significantly associated with postoperative CME at 3 months.
Common risk factors for CME were identified in previous reports22,23,24. These risks include uveitis, diabetic retinopathy, retinal vein occlusion, age-related macular degeneration, retinitis pigmentosa, vitreous traction, cataract surgery, and perioperative use of prostaglandin analogues. Multiple studies showed that inflammation has a key role in the onset of CME after cataract surgery, particularly because of its potential for disrupting blood–retinal and blood–aqueous barriers22,25,26.
Compared with a shorter duration of surgery, a longer duration of surgery may lead to more severe postoperative ocular inflammation. Additionally, eyes with a lower preoperative number of corneal endothelial cells may have broken blood–retinal and blood–aqueous barriers, facilitating the onset of postoperative ocular inflammation. Postoperative transient ocular hypotension may also contribute to postoperative ocular inflammation. In this study, ocular inflammation was quantified using a laser flare meter. Although flare data were only available for 57 eyes in the Yamane technique group, we found no difference in ocular inflammation between eyes with and without postoperative CME.
Notably, pseudoexfoliation was a predictive factor for the development of postoperative CME. Previously, Leshno et al. reported that the ocular surface temperature was higher in eyes with primary open angle glaucoma and pseudoexfoliation glaucoma than in healthy eyes, suggesting that glaucoma (e.g., pseudoexfoliation) affects ocular inflammation27.
The rate of postoperative CME was higher in the Yamane technique group than in the conventional technique group. The IOL flange may be harder and larger than sutures; thus, the portion of IOL flange in the ciliary body could cause chronic inflammation. However, additional data regarding ocular inflammation (e.g., flare) are needed to confirm this hypothesis.
To avoid postoperative CME, clinicians must focus on surgical skills and avoid causing increased ocular inflammation (e.g., via damage to the iris). When postoperative CME occurs, rapid management is essential. In Hyogo Medical University (excluding data from other institutions), subtenon triamcinolone acetonide injection has been an effective approach.
There were some limitations in this study. First, we used a retrospective design; thus, some data may have differed among centres because they were not collected in a standardised manner. For example, only three institutions had a system for flare measurement, and multiple surgeons performed the procedures in this study. Second, the follow-up duration was limited to 3 months; the use of a longer follow-up period may have substantially altered our conclusions. Third, the study period ranged from January 2019 to January 2021; surgical practices may have changed during that time, and such changes may have contributed to bias in the results. Fourth, individual surgeons’ preferences concerning postoperative steroids/non-steroidal anti-inflammatory drugs might have influenced their selected surgical technique; this influence may have led to bias in the study results.
In conclusion, although the Yamane technique is popular among retinal surgeons because of its convenience for SFIOL, our findings suggest that it carries an increased risk of postoperative CME, compared with the conventional suture method. Therefore, careful management of postoperative CME is needed after SFIOL.
Data availability
All data generated or analysed during this study are included in this published article and its Supplementary Information file.
References
Yamane, S., Inoue, M., Arakawa, A. & Kadonosono, K. Sutureless 27-gauge needle-guided intrascleral intraocular lens implantation with lamellar scleral dissection. Ophthalmology 121, 61–66. https://doi.org/10.1016/j.ophtha.2013.08.043 (2014).
Yamane, S., Sato, S., Maruyama-Inoue, M. & Kadonosono, K. Flanged intrascleral intraocular lens fixation with double-needle technique. Ophthalmology 124, 1136–1142. https://doi.org/10.1016/j.ophtha.2017.03.036 (2017).
Hoffman, R. S., Fine, I. H., Packer, M. & Rozenberg, I. Scleral fixation using suture retrieval through a scleral tunnel. J. Cataract Refract. Surg. 32, 1259–1263. https://doi.org/10.1016/j.jcrs.2006.02.065 (2006).
Akimoto, M., Taguchi, H. & Takahashi, T. Using catheter needles to deliver an intraocular lens for intrascleral fixation. J. Cataract Refract. Surg. 40, 179–183. https://doi.org/10.1016/j.jcrs.2013.12.009 (2014).
Ohta, T., Toshida, H. & Murakami, A. Simplified and safe method of sutureless intrascleral posterior chamber intraocular lens fixation: Y-fixation technique. J. Cataract Refract. Surg. 40, 2–7. https://doi.org/10.1016/j.jcrs.2013.11.003 (2014).
Wang, W., Syed, R., Hadayer, A., Jusufbegovic, D. & Schaal, S. Twenty-seven-gauge vitrectomy-assisted four-point scleral fixation of intraocular lens in the absence of capsular support. Retina 36, 1605–1608. https://doi.org/10.1097/IAE.0000000000001148 (2016).
Walsh, M. K. Sutureless trocar-cannula-based transconjunctival flanged intrascleral intraocular lens fixation. Retina 37, 2191–2194. https://doi.org/10.1097/IAE.0000000000001593 (2017).
Hu, Z. X. et al. Sutureless intrascleral haptic-hook lens implantation using 25-gauge trocars. J. Ophthalmol. 2018, 9250425. https://doi.org/10.1155/2018/9250425 (2018).
John, T., Tighe, S., Hashem, O. & Sheha, H. New use of 8 – 0 polypropylene suture for four-point scleral fixation of secondary intraocular lenses. J. Cataract Refract. Surg. 44, 1421–1425. https://doi.org/10.1016/j.jcrs.2018.08.008 (2018).
Kataoka, T. & Kamei, M. Silicone microtube-assisted scleral fixation of a posterior chamber intraocular lens. Retina 38, S146–S153. https://doi.org/10.1097/IAE.0000000000002143 (2018).
Aaltonen, P., Oskala, P. & Immonen, I. Outcomes of intraocular lens scleral fixation with the friction knot technique. Acta Ophthalmol. 97, e506–e513. https://doi.org/10.1111/aos.13931 (2019).
Gelman, R. A. & Garg, S. Novel Yamane technique modification for haptic exposure after glued intrascleral haptic fixation. Am. J. Ophthalmol. Case Rep. 14, 101–104. https://doi.org/10.1016/j.ajoc.2019.03.009 (2019).
Hadayer, A., Puri, S., Fassbender Adeniran, J., Wang, W. & Kaplan, H. J. Minimally invasive ab interno four-point scleral fixation of intraocular lens. Retina 39, S21–S23. https://doi.org/10.1097/IAE.0000000000002138 (2019).
Sugiura, T., Kaji, Y. & Tanaka, Y. Ciliary sulcus suture fixation of intraocular lens using an auxiliary device. J. Cataract Refract. Surg. 45, 711–718. https://doi.org/10.1016/j.jcrs.2019.01.021 (2019).
Thanos, A., Lau-Sickon, L. K., Wolfe, J. D. & Hassan, T. S. Three port sutureless posterior chamber intraocular lens intrascleral fixation: A novel approach. Retina 39, 16–20. https://doi.org/10.1097/IAE.0000000000001925 (2019).
Walia, S., Kashyap, S., Bhaisare, V., Rawat, P. & Kori, N. Novel technique of sutureless glueless scleral fixated intraocular lens (SFIOL). Indian J. Ophthalmol. 67, 64–68. https://doi.org/10.4103/ijo.IJO_447_18 (2019).
Bonnell, A. C., Polo, R. N., Shah, S. P., Fine, H. F. & Prenner, J. L. One-year outcomes of a novel surgical technique for sutureless intrascleral fixation of a three-piece intraocular lens using a 30-gauge needle. Retina 40, 1148–1152. https://doi.org/10.1097/IAE.0000000000002560 (2020).
Chantarasorn, Y., Pokawattana, I., Silpa-Archa, S., Ratprasatporn, N. & Saovaprut, C. Relay intrascleral 6 – 0 polypropylene-assisted intraocular lens fixation: A retrospective comparison with modified Yamane Technique. Retina 44, 455–464. https://doi.org/10.1097/IAE.0000000000003971 (2024).
Drummond, S. C. et al. Scleral fixated secondary IOLs: An outcomes comparison between the Yamane and gore-tex-sutured techniques. Opthalmic Surg. Lasers Imaging Retin. 55, 384–390. https://doi.org/10.3928/23258160-20240226-01 (2024).
Kim, J., Lee, P. Y., Park, M. S., Cho, B. J. & Kwon, S. Comparison of outcomes between modified double-flanged sutureless scleral fixation and conventional sutured scleral fixation. Sci. Rep. 14, 16111. https://doi.org/10.1038/s41598-024-66762-y (2024).
Lange, C., Feltgen, N., Junker, B., Schulze-Bonsel, K. & Bach, M. Resolving the clinical acuity categories hand motion and counting fingers using the Freiburg Visual Acuity Test (FrACT). Graefes Arch. Clin. Exp. Ophthalmol. 247, 137–142. https://doi.org/10.1007/s00417-008-0926-0 (2009).
Holló, G., Aung, T., Cantor, L. B. & Aihara, M. Cystoid macular edema related to cataract surgery and topical prostaglandin analogs: Mechanism, diagnosis, and management. Surv. Ophthalmol. 65, 496–512. https://doi.org/10.1016/j.survophthal.2020.02.004 (2020).
Chu, C. J. et al. Risk factors and incidence of macular edema after cataract surgery: A database study of 81984 eyes. Ophthalmology 123, 316–323. https://doi.org/10.1016/j.ophtha.2015.10.001 (2016).
Henderson, B. A. et al. Clinical pseudophakic cystoid macular edema. Risk factors for development and duration after treatment. J. Cataract Refract. Surg. 33, 1550–1558. https://doi.org/10.1016/j.jcrs.2007.05.013 (2007).
Cho, H. & Madu, A. Etiology and treatment of the inflammatory causes of cystoid macular edema. J. Inflamm. Res. 2, 37–43. https://doi.org/10.2147/JIR.S5706 (2009).
Grzybowski, A., Sikorski, B. L., Ascaso, F. J. & Huerva, V. Pseudophakic cystoid macular edema: Update 2016. Clin. Interv Aging. 11, 1221–1229. https://doi.org/10.2147/CIA.S111761 (2016).
Leshno, A. et al. Ocular surface temperature differences in glaucoma. Eur. J. Ophthalmol. 32, 1518–1524. https://doi.org/10.1177/11206721211023723 (2022).
Acknowledgements
We thank Ryan Chastain-Gross, Ph.D., from Edanz (https://jp.edanz.com/ac) for editing a draft of this manuscript.
Funding
None.
Author information
Authors and Affiliations
Contributions
Hiroto Ishikawa: Conceptualisation, Methodology, Formal analysis and investigation, Writing—original draft preparation, Writing—review and editing, Resources; Kazutaka Uchida: Methodology, Formal analysis and investigation, Writing—original draft preparation; Fumi Gomi: Writing—review and editing, Funding acquisition, Supervision; Hiroto Terasaki: Resources; Masashi Kakinoki: Resources; Tatsuya Jujo: Resources; Yutaka Yamada: Resources; Masahiko Sugimoto: Resources; Hisashi Fukuyama: Resources; Taiji Sakamoto: Supervision; Masahito Ohji: Supervision; Hitoshi Takagi: Supervision; Yoshinori Mitamura: Supervision; Yoshihiro Takamura: Supervision; Mineo Kondo: Supervision; Shigeo Yoshida: Supervision.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Ishikawa, H., Uchida, K., Terasaki, H. et al. Cystoid macular oedema after flanged intraocular lens scleral fixation using the Yamane technique: a multicentre cohort study. Sci Rep 15, 811 (2025). https://doi.org/10.1038/s41598-025-85370-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-025-85370-y
