
Abstract
Fatigue has gradually become an important factor affecting the health and work quality of healthcare workers. However, the occurrence of fatigue and related factors in the context of heavy workloads and strained doctor-patient relationships have not been adequately studied in Northeast China. The current study aims to assess the situation of fatigue among healthcare workers in tertiary general hospitals in Northeast China, and to further analyze the influencing factors of fatigue among healthcare workers (doctors and nurses as a whole), doctors and nurses from various perspectives. A cross-sectional survey was conducted among healthcare workers who met the inclusion criteria in two tertiary general hospitals in Dalian, Liaoning Province, Northeast China. The survey data collected in the structured questionnaire include fatigue, general demographic characteristics, work situation, perceived stress, insomnia symptoms, workplace violence, anxiety symptoms, depressive symptoms, family function, and doctor-patient relationship. A binary logistic regression model was applied to analyze the independent influencing factors of fatigue. A total of 1004 healthcare workers were included in this study (503 doctors and 501 nurses). The prevalence of fatigue was 53.9% for healthcare workers, with rates of 52.3% for doctors, and 55.5% for nurses. Binary logistic regression analysis showed that health status, perceived stress, insomnia symptoms, anxiety symptoms, and doctor-patient relationship were influencing factors of fatigue among healthcare workers, doctors, and nurses. Chronic pain was an influencing factor for fatigue among healthcare workers and nurses. Depressive symptoms were an influencing factor for fatigue for healthcare workers and doctors. Night shift frequency was an influencing factor for fatigue for nurses. In Northeast China, tertiary general hospitals have a relatively high prevalence of fatigue among healthcare workers, especially among nurses. Fatigue was influenced by various factors such as health status, perceived stress, insomnia symptoms, anxiety symptoms, and doctor-patient relationships. It is necessary to raise awareness of fatigue among healthcare workers, particularly healthcare workers with risk factors, and to develop targeted and effective intervention measures aimed at reducing fatigue.
Similar content being viewed by others

Introduction
Fatigue is defined as a subjective unpleasant symptom, encompassing a spectrum from tiredness to exhaustion, with its nature ranging from acute to chronic, resulting in an overall condition that is difficult to alleviate. It can cause decreased energy and impairment of physical and cognitive functions, which would affect and individual’s normal capability to live and work1. It is a common modern occupational disease, primarily characterized by a loss of enthusiasm, empathy, and sense of responsibility towards work, or even developing aversion towards work2. Fatigue can also reduce attendance rates and may disrupt normal behavioral abilities in the workplace3. More than 60% of the general working population feel tired or exhausted after a day’s work4.
According to the World Health Statistics 2022 released by World Health Organization (WHO), the density of doctors and nurses per 10,000 people in China is only 22.3 and 30.8, which is significantly lower compared to developed countries5. Chinese healthcare workers generally work long hours in a common working environment and their workload was increased even more during public health emergencies leading to a high prevalence of occupational fatigue6. A previous study at Taiwan’s Cheng Hsin General Hospital found that the prevalence for personal fatigue was 28.2% at moderate risk and 12.5% at high risk among medical professionals aged 30 and above, while for the work-related fatigue, the prevalence was 24.9% at moderate risk and 14.2% at high risk7. A survey conducted among healthcare workers during the COVID-19 outbreak in Yangzhou, China revealed a prevalence of mild fatigue was 55.36%, moderate fatigue was 18.03%, and severe fatigue was 3.86%6. A study on aeromedical doctors transporting critically ill patients abroad showed a significant increase in fatigue during the task8. In 2019, a survey of 141 surgical technicians selected through random sampling at Mazandaran Medical University Hospital showed that 82.2% of them had moderate to severe fatigue9. Although more and more literature is capturing the fatigue situation among healthcare workers, there is still relatively lack of attention to fatigue among healthcare workers in China. Fatigue among healthcare workers can lead to physical weakness and mental sluggishness, which can affect their ability to work and study. Prolonged fatigue can also affect immune system and increase the risk of disease and sudden death10. In addition, fatigue can have a negative impact on the cognitive function of healthcare workers, reducing with alertness and logical reasoning ability11. These effects pose significant dangers for healthcare works that requires high levels of concentration and precise judgment, and may even lead to medical errors, impacting the medical quality and patient safety. Therefore, it is important to explore the influencing factors of fatigue in healthcare workers and develop relevant intervention strategies.
Fatigue is typically caused by physiological, cognitive, emotional, and sensory factors, and can also be the result of a high workloads and insufficient time for recovery12. Research has shown that high levels of perceived stress are predictors of fatigue risk13. During the COVID-19 pandemic in Wuhan, different perceived health statuses exhibited different levels of fatigue, and different levels of resilience in healthcare workers had a statistically significant impact on fatigue14. It is worth noting that the longer the working hours of frontline healthcare workers, the higher their level of fatigue, as mandatory long working hours and shifts can lead to long-term fatigue due to impaired work recovery15,16. Previous studies have reported risk factors and protective factors for fatigue in healthcare workers; however, more comprehensive analyses of fatigue-related factors are needed, as many studies have only analyzed a few aspects. Literature has reported that nurses who have experienced severe workplace violence are more likely to develop chronic fatigue syndrome17. In addition, pain intensity, pain spread and fatigue indices were highly correlated in patients with chronic pain18. More importantly, in the healthcare field, doctor-patient relationships have a profound impact on the smooth conduct of medical activities and social harmony, and the quality of doctor-patient relationships directly impacts the physical and mental health of healthcare workers19. Therefore, the relationship between these aspects and healthcare workers fatigue needs to be studied more extensively.
Previous studies in China often treated doctors and nurses as a unified entity for research purpose, with generally small sample sizes. Doctors and nurses have different job natures, responsibilities, and social statuses. Studies investigating the influencing factors of fatigue in doctors and nurses separately in the same context are lacking in China. In addition, the prevalence and influencing factors of fatigue among healthcare workers may vary between different countries and regions. Different regions need to establish intervention strategies that are tailored to the healthcare workers in their respective regions to provide interventions that are more responsive to the unique needs of healthcare workers in their regions. However, there is still a lack of relevant studies in Northeast China. Therefore, this study assessed the current situation of fatigue among healthcare workers (doctors and nurses as a whole), doctors, and nurses in the context of strained doctor-patient relationships and heavy workloads, and conducted an in-depth analysis of various factors related to fatigue among healthcare workers, doctors, and nurses in terms of demographic characteristics, work situations, perceived stress, insomnia symptoms, workplace violence, anxiety symptoms, depressive symptoms, family function, and doctor-patient relationships. Understanding these factors is crucial for developing targeted intervention measures to better support vulnerable healthcare workers and mitigate the negative impacts on the effective operation of the healthcare systems.
Methods
Study design
A cross-sectional survey was conducted from February 2024 to March 2024 in two tertiary general hospitals in Dalian, Liaoning Province, Northeast China.
Participants
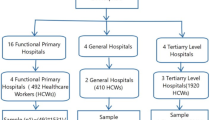
A questionnaire survey was conducted by random sampling method among healthcare workers who met the inclusion criteria in two tertiary general hospitals in Northeast China. The inclusion criteria were as follows: (1) healthcare workers aged 18 years or older; (2) healthcare workers engaged in clinical medical work or nursing work for one year or more; (3) healthcare workers without a history of psychiatric diagnosis; (4) healthcare workers capable of adhering to the research process and consenting participate in this study. The investigator went to the department of healthcare workers to distribute the questionnaire to the participants, and the purpose and confidentiality of the survey were clearly stated. The investigator waited for the participants to fill out the questionnaire and was responsible for guiding the participants. Participants filled out the questionnaires themselves, with an average time of about 15–20 min. All questionnaires were retrieved on the spot. The minimum required sample size was calculated by the single population proportion formula. Due to the lack of relevant studies in Northeast China, a prevalence of fatigue of 50%, 95% confidence interval (CI), a margin error of 5%, and a non-response rate of 20% were used in order to obtain an adequate sample size. The minimum sample size required was calculated to be 461. Considering invalid questionnaires and in order to obtain more reliable results, we decided to distribute a total of 1,020 questionnaires (510 for doctors and 510 for nurses). All respondents signed informed consent forms before the questionnaire survey. Sixteen invalid questionnaires were excluded during the collection due to illogical responses or missing information. Finally, 1004 valid questionnaires with no missing items (503 from doctors and 501 from nurses) were collected, with a valid response rate of 98.4%.
Ethics procedure
This study was conducted in accordance with the Declaration of Helsinki. This study was approved by the Ethics Committee of the First Affiliated Hospital of Dalian Medical University. All participants provided written informed consent after the investigator presented the purpose of the study. Each participant volunteered to participate in this study and the information filled out was confidential and anonymous.
Data collection
A structured questionnaire self-developed by reviewing a large number of relevant research literature and consulting experts in related fields was used to collect data. A pre-survey was conducted in healthcare organizations prior to actual data collection. The questionnaire was modified and supplemented based on feedback to ensure its scientific validity. The questionnaire included general demographic characteristics, work situation, fatigue, perceived stress, insomnia symptoms, workplace violence, anxiety symptoms, depressive symptoms, family function, and doctor-patient relationship. The data were collected by an established survey team. Each member of the team received unified training on how to collect data and the correct practices to follow to ensure consistent and standardized data collection.
General demographic characteristics include gender (male, female), age (< 30 years, 30–40 years, > 40 years), educational status (bachelor below, bachelor, master or above), per capita monthly income (< 5,000 yuan, 5,000–10,000 yuan, > 10,000 yuan), chronic pain (yes, no), chronic disease (yes, no), smoking (yes, no), alcohol consumption (yes, no), and health status (poor, fair, good). Work situation included years of work experience (≤ 5 years, 6–15 years, > 15 years), number of night shifts per month (≤ 3 times, > 3 times), weekly work hours (≤ 40 h, > 40 h), and adverse work events (yes, no).
Fatigue was measured using the Fatigue Scale-14 (FS-14)20. FS-14 was originally developed by Chalder et al. in 1992 and is a widely recognized fatigue assessment tool20. It is designed to assess the severity of recent fatigue in the study subjects. It consists of 14 items, including two dimensions of physical fatigue (items 1 to 8) and mental fatigue (items 9 to 14). Each item has two options (0 = no, 1 = yes) with a total score ranging from 0 to 14. A higher total score indicates more severe fatigue. Fatigue is considered to occur when the total score is greater than or equal to 721. FS-14 has been proven to have good reliability and validity22,23,24. In the current study, this scale demonstrated high internal consistency (Cronbach’s α = 0.806).
Perceived stress levels were measured by the Perceived Stress Scale-10 (PSS-10)25,26. PSS was originally developed by Cohen et al. in 1983 with 14 items and was modified to form 10 items by Cohen and Williamson in 198825,26. It is used to assess the level of perceived stress in the past month. The scale consists of 6 negative items and 4 positive items. The negative items assess the sense of loss of control and negative emotional reactions, while the positive items assess the ability to deal with existing stressors. The scale was used a 5-point Likert scale, where 0–4 represent “never to almost always”. The total score ranges from 0 to 40, with higher scores indicating higher levels of perceived stress. A total score greater than or equal to 15 was defined as high perceived stress27. PSS-10 has been widely used28,29. In the current study, this scale demonstrated good internal consistency (Cronbach’s α = 0.768).
Insomnia symptoms were assessed using the Insomnia Severity Index (ISI)30. ISI consists of 7 items, including severity of sleep-onset, sleep maintenance, early morning awakening problems, sleep dissatisfaction, interference of sleep difficulties with daytime functioning, noticeability of sleep problems and distress caused by the sleep difficulties during daytime and night-time31. The scale uses a 5-point Likert scale to rate 7 self-reported items, with scores ranging from 0 to 4. The total score is the sum of the scores for each item, ranging from 0 to 28. The suggested detection threshold for insomnia symptoms on this scale is 7 points30. Therefore, in this study, a total score of more than 7 was considered as having symptoms of insomnia. ISI has demonstrated good reliability and validity32,33. The scale also showed high internal consistency in this study (Cronbach’s α = 0.926).
Workplace violence was measured using the Workplace Violence Scale (WVS)34. The scale was developed by Schat et al. and translated and revised by Wang Peixi in 200634. It was used to evaluate the frequency of workplace violence experienced by the study participants in the past one year. The scale consists of 5 items: physical assault, emotional abuse, threats and intimidation, verbal harassment, and physical harassment. Each item was rated on a 4-point Likert scale (0: no violence, 1: once, 2: 2–3 times, 3: 4 or more times). The total score of the scale is the sum of the scores for each item, with higher scores indicating a higher frequency of workplace violence. A score of 0 indicates no workplace violence, while a score greater than 0 indicates the presence of workplace violence34. In the current study, this scale exhibited good internal consistency (Cronbach’s α = 0.746).
Anxiety symptoms were measured using the Generalized Anxiety Disorder Scale (GAD-7)35. The scale is used to assess the frequency of anxiety symptoms in individuals over the past two weeks. It consists of 7 items on a 4-point scale from 0 to 3. The total score ranges from 0 to 21, with higher scores indicating more pronounced anxiety symptoms in the study population. The recommended screening threshold for anxiety symptoms on this scale is 7, with a total score 7 or higher indicating the presence of anxiety symptoms36. This scale has been validated to assess anxiety in participants37. In the current study, the scale exhibited high internal consistency (Cronbach’s α = 0.928).
Depressive symptoms were measured using the Patient Health Questionnaire-9 (PHQ-9)38. It assesses the degree to which the study participants were troubled by depressive symptoms in the last two weeks. It consists of 9 items, each scored on a Likert scale from 0 (not at all) to 3 (almost every day). The total score of the 9 items yields the PHQ-9 total score, ranging from 0 to 27. The higher the score, the greater the degree of depressive symptoms present in the study population. The recommended threshold for depressive symptoms on this scale is 1039,40. Therefore, in this study, a total score greater than or equal to 10 is defined as the presence of depressive symptoms. PHQ-9 has been well applied in the Chinese population and has good reliability and validity40,41. In the current study, the scale exhibited high internal consistency (Cronbach’s α = 0.897).
Family function was measured using the Family Adaptation Partnership Growth Affection and Resolve index (APGAR) developed by Smilkstein in 197842. The questionnaire consists of five items: adaptability, partnership, growth, affection and resolve, each representing an aspect of family function. A 3-point scale was used, i.e., 2 points for “always”, 1 point for “sometimes”, and 0 point for “hardly never”. The total score ranges from 0 to 10, with higher scores indicating better family function. Total score of 0–3 indicate severe family dysfunction, 4–6 indicate moderate family dysfunction, and 7–10 indicate good family function43. In the current study, this scale exhibited high internal consistency (Cronbach’s α = 0.915).
The doctor-patient relationship was measured using the 10-item Difficult Doctor-Patient Relationship Questionnaire (DDPRQ-10)44,45, which consists of 10 items across 3 dimensions: “subjective feelings of the doctor” (2 items), “objective issues of patient behavior” (4 items), and “combination of patient behavior and subjective feelings of the doctor” (4 items)46. Each item is rated on a 5-point Likert scale ranging from 1 (not at all) to 5 (very much), with a total score ranging from 10 to 50, with higher scores indicating more tension in the doctor-patient relationship46. In this study, a total score greater than or equal to the mean score was considered indicative of a poor doctor-patient relationship. The questionnaire has been widely used46. In the current study, the questionnaire exhibited high internal consistency (Cronbach’s α = 0.815).
Data processing and analysis
The questionnaires were checked for data integrity and consistency at the time of recovery, and complete and error-free questionnaires were coded. Double entry was used to enter data into the database created by EpiData version 3.1 (EpiData Association, Odense, Denmark) software to ensure accuracy. The data were exported to SPSS version 21.0 (IBM Corporation, Armonk, State of New York) for statistical analysis. Mean and standard deviation were calculated for continuous data, while frequency and percentage were used for categorical data. Chi-square tests were applied to compare the incidence rates of healthcare worker fatigue across demographic characteristics, work situation, perceived stress, insomnia symptoms, workplace violence, anxiety symptoms, depressive symptoms, family function, and doctor-patient relationship. Variables with statistically significant differences in univariate analyses were included in binary logistic regression models to assess the independent effects of each variable after adjusting for potential confounders. Prior conducting binary logistic regression, we tested for collinearity among predictor variables and found that the variance inflation factor (VIF) for each variable was less than 10, with tolerance was much greater than 0.1. Therefore, there was no collinearity among all predictor variables. All comparisons were two-sided and P < 0.05 was considered statistically significant.
Results
Occurrence of fatigue
A total of 1004 healthcare workers were included in this study, including 503 doctors and 501 nurses. The prevalence of fatigue was 53.9% among healthcare workers, 52.3% among doctors and 55.5% among nurses.
Characteristics of the study population
Among the 1004 healthcare workers, 72.7% were female and more than half (50.2%) were aged 30–40 years. More than one-third (47.4%) of the healthcare workers had 6–15 years of work experience. More than half (52.3%) of the healthcare workers worked more than 3 night shifts per month, and the majority (70.2%) of the healthcare workers experienced chronic pain. Healthcare workers who rated their health as fair accounted for 60.3%, while more than half (56.9%) worked ≤ 40 h per week. 51.4% of healthcare workers perceived high levels of stress, and nearly half (49.5%) had symptoms of insomnia. Anxiety and depressive symptoms were found in 27.3% and 13.0% of healthcare workers, respectively. The majority of healthcare workers (67.8%) had good family function and more than half (53.6%) perceived poor doctor-patient relationship. See Table 1 for details.
Relationship between the variables of healthcare works, doctors, and nurses and fatigue
Among 1004 healthcare workers, there were significant differences in the incidence of fatigue by age, years of work experience, number of night shifts per month, chronic pain, chronic disease, health status, weekly working hours, adverse work events, perceived stress, insomnia symptoms, workplace violence, anxiety symptoms, depressive symptoms, family function, and doctor-patient relationship (P < 0.05). Among 503 doctors, significant differences in the incidence of fatigue were observed among different levels of chronic pain, chronic disease, health status, weekly working hours, perceived stress, insomnia symptoms, workplace violence, anxiety symptoms, depressive symptoms, family function, and doctor-patient relationship (P < 0.05). Among 501 nurses, significant differences in the incidence of fatigue were observed among different age groups, years of work experience, number of night shifts per month, chronic pain, chronic disease, health status, weekly working hours, perceived stress, insomnia symptoms, workplace violence, anxiety symptoms, depressive symptoms, family function, and doctor-patient relationships (P < 0.05). See Table 2 for details.
Binary logistic regression analysis of factors influencing fatigue in healthcare works
Binary logistic regression analyses indicated that absence of chronic pain (OR = 0.552, 95% CI: 0.364–0.750), good health status (OR = 0.172, 95% CI: 0.091–0.326), and fair health status (OR = 0.356, 95% CI: 0.200-0.631) were protective factors related to fatigue among healthcare workers. Higher levels of perceived stress, (OR = 1.980, 95% CI: 1.430–2.743), insomnia symptoms (OR = 1.755, 95% CI: 1.266–2.433), anxiety symptoms (OR = 3.356, 95% CI: 2.149–5.240), depressive symptoms (OR = 2.201, 95% CI: 1.057–4.583), and poor doctor-patient relationship (OR = 2.236, 95% CI: 1.621–3.085) were risk factors related to fatigue among healthcare workers. See Table 3 for details.
Binary logistic regression analysis of factors influencing fatigue among doctors
Binary logistic regression analysis showed good health status (OR = 0.206, 95% CI: 0.081–0.525) was a protective factor associated to fatigue among doctors. Higher level of perceived stress, (OR = 1.893, 95% CI: 1.187–3.021), insomnia symptoms (OR = 1.603, 95% CI: 1.008–2.549), anxiety symptoms (OR = 3.719, 95% CI: 1.928–7.173), depressive symptoms (OR = 2.960, 95% CI: 1.029–8.510), and poor doctor-patient relationship (OR = 2.652, 95% CI: 1.673–4.203) were identified as risk factors associated to fatigue among doctors. See Table 4 for details.
Binary logistic regression analysis of factors influencing fatigue among nurses
Binary logistic regression analysis indicated that good health status (OR = 0.156, 95% CI: 0.064–0.381) and fair health status (OR = 0.279, 95% CI: 0.128–0.610), and the absence of chronic pain (OR = 0.416, 95% CI: 0.244–0.709) were protective factors associated to fatigue among nurses. Number of night shifts per month > 3 (OR = 1.611, 95% CI: 1.007–2.578), higher level of perceived stress, (OR = 1.954, 95% CI: 1.222–3.125), insomnia symptoms (OR = 1.782, 95% CI: 1.114–2.850), anxiety symptoms (OR = 3.158, 95% CI: 1.690–5.898), and poor doctor-patient relationship (OR = 1.793, 95% CI: 1.129–2.848) were risk factors associated to fatigue among nurses. See Table 5 for details.
Discussion
This study assessed the current situation of fatigue among healthcare workers, doctors and nurses in tertiary general hospitals in Northeast China in the context of high workload and tense doctor-patient relationships, and comprehensively explored the factors related to fatigue among healthcare workers, doctors and nurses. To our knowledge, this is the first study on fatigue among healthcare workers in Northeast China, which will provide guidance for the development of intervention measures for fatigue among healthcare workers that are tailored to the region. The results of this study show that 53.9% of healthcare workers in Northeast China experience fatigue, which is higher than the fatigue prevalence of 4.7% among healthcare workers in a tertiary hospital in Bangalore, India47; Higher than the prevalence rates of personal and work-related fatigue among medical staff in Cheng Hsin General Hospital, Taiwan, which are 41.4% and 39.1% respectively7; but lower than the prevalence of fatigue among frontline healthcare workers in Ningbo during the COVID-19 pandemic, where it reached 82%48. The above differences may be attributed to research design, geographic factors, and social cultural. The incidence of fatigue among healthcare workers in Northeast China is relatively high. Therefore, the development of targeted and effective interventions to alleviate fatigue is urgently needed. In addition, this study also found that the incidence of fatigue is higher among nurses (55.5%) than that of doctors (52.3%). This is consistent with previous studies that mental health problems such as fatigue are particularly prevalent among nurses49. This may be due to the fact that nurses have longer and more extensive contact with patients than doctors, engage in frequent and unpredictable daily work, and must often manage patients and their families during emergencies and meet their expectations49. Moreover, 93.2% of nurses are women, and certain gender-specific physiological factors (e.g., menstruation and pregnancy) as well as social backgrounds and living conditions (e.g., employment and childcare) may contribute to women being more susceptible to fatigue than men50. Therefore, more attention should be given to nurses when developing interventions, and the focus should be on increasing awareness of nurse fatigue and actively intervene with its risk factors.
This study found that health status is a factor influencing fatigue of healthcare workers, doctors, and nurses. A study in the UK showed that fatigue is strongly associated to physical and mental health indicators51, which is consistent with our results. Healthcare workers can enhance their physical fitness through exercise to promote physical and mental health52. The results of this study show that perceived stress, is a predictor of fatigue in healthcare workers, doctors, and nurses. A study in Iran shows that high job stress significantly affects the level of fatigue status of nurses, and the impact of job stress on fatigue would be more pronounced if social support is low53, which is consistent with the results of this study. Relatives and hospital leaders should provide higher social support to healthcare workers to reduce the occurrence of fatigue. This study also found that healthcare workers, doctors, and nurses with insomnia symptoms are more prone to fatigue. Previous studies have also confirmed our findings that sleep duration is a significant predictor of fatigue54.Therefore, timely detection of sleep problems among healthcare workers and provide appropriate treatment and intervention are essential. Relevant departments should rationalize the frequency of night shifts to reduce the sleep quality problems of healthcare workers caused by rotating shifts. Healthcare workers themselves should also develop good sleep habits. Interventions and strategies such as encouraging physical exercise, cognitive-behavioral therapy, providing sleep education programs, and improving the work and sleep environments should also be considered to improve the sleep quality of healthcare workers55,56,57. Some studies have shown that anxiety is a significant predictor of fatigue58. This is consistent with our findings, anxiety symptoms are an independent influencing factor for the fatigue among healthcare workers, doctors, and nurses. These results emphasize the importance of implementing targeted mental health interventions to address anxiety among healthcare workers, and it is crucial to include them in management on occupational health and safety. It has been reported in the literature that the patient-doctor relationships play an important role in providing high quality healthcare59. Tense patient-doctor relationships means may lead to more complaints and disputes, affecting the healthcare workers’ job satisfaction and motivation, and having a negative impact on mental health60. This aligns with our findings that poor doctor-patient relationships are more likely to experience fatigue among healthcare workers, doctors, and nurses. Therefore, doctor-patient communication should be strengthened, the quality of medical services should be improved, and the mechanism for handling medical disputes should be refined, etc., in order to alleviate the tension in the doctor-patient relationships61, hereby reducing fatigue among healthcare workers.
Results from a longitudinal study conducted among children and adolescents show that students with chronic pain had a significantly higher prevalence of severe fatigue than students without chronic pain62.Similar to the findings of previous studies, our study found that chronic pain is an independent influencing factor for the fatigue of healthcare workers and nurses. Healthcare workers often endure high work intensity, frequently requiring prolonged maintenance of certain positions such as standing, bending or carrying heavy loads, which can lead to joint and muscle overstrain or injury, resulting chronic pain, which will further exacerbate the feelings of fatigue without adequate rest and recovery. Therefore, healthcare workers need to adjust their working posture correctly and engage in appropriate physical activity and rest. This study also found that healthcare workers and doctors with depressive symptoms are more prone to fatigue, which is similar to the results of previous study results, and depression is still significantly associated with fatigue in patients with excessively sleep during the day63. Healthcare workers under extreme work pressure, complex medical problems and high-risk medical tasks, which can easily lead to depressive moods, resulting low energy, loss of interest, sleep disorders, etc., exacerbating feelings of fatigue. Providing psychological counseling can alleviate depressive moods among healthcare workers and promote physical and mental health. The study also found that the number of night shifts per month is an influential factor in nurse fatigue. Similar to previous studies, evidence-based research indicates that especially in situations where schedules violate the human circadian rhythm, there is an increase in occupational accidents and illnesses among employees64. Therefore, medical institutions should reasonably arrange the working time of nurses, allocate manpower appropriately, optimize night shift systems, and alleviate fatigue of nurses caused by night shifts.
Although valuable information has been found in the current study, there are some limitations that require further explanation. Firstly, due to the nature of the cross-sectional survey design, causality between the variables could not be established. A longitudinal design would be required in order to establish causality between these variables in the future. Secondly, the sample in this study only included healthcare workers from 2 tertiary general hospitals in the same region, limiting the generalizability of the study results. Future studies should include samples from different regions. Lastly, only doctors and nurses were included in this study; other types of personnel working in the hospital were not included. Future studies should expand the scope of participants.
Conclusion
In summary, the percentage of fatigue occurs among healthcare workers in tertiary general hospitals in Northeast China is relatively high. Health status, perceived stress, insomnia symptoms, anxiety symptoms, and doctor-patient relationship are common influencing factors for fatigue among healthcare workers, doctors, and nurses. Chronic pain is an independent influencing factor for fatigue among healthcare workers and nurses. Depressive symptoms are an influencing factor for healthcare workers and doctors. The number of night shifts per month is an influencing factor for fatigue among nurses. Therefore, awareness of healthcare workers fatigue should be raised. There is an urgent need to develop targeted and effective intervention measures aimed at reducing fatigue among healthcare workers, while also pay more attention to doctors and nurses with risk factors.
Data availability
The raw data supporting the conclusions of this article will be made available by the corresponding author, without undue reservation.
References
Min, A., Min, H. & Hong, H. C. Work schedule characteristics and fatigue among rotating shift nurses in hospital setting: An integrative review. J. Nurs. Adm. Manag. 27 (5), 884–895 (2019).
Steege, L. M. & Pinekenstein, B. Addressing occupational fatigue in nurses: A risk management model for nurse executives. J. Nurs. Adm. 46 (4), 193–200 (2016).
Seol, M. J., Lee, B. S. & Lee, S-K. Effects of labor intensity and fatigue on sleep quality of clinical nurses. J. Korean Acad. Nurs. Adm. 24(4), 276 (2018).
Bláfoss, R. et al. Physical workload and bodily fatigue after work: Cross-sectional study among 5000 workers. Eur. J. Pub. Health. 29 (5), 837–842 (2019).
Organization, W. H. World health statistics 2022: Monitoring health for the SDGs, sustainable development goals (2023).
Tang, X. et al. Mental health and fatigue status of the medical workforce during the COVID-19 outbreak in the Yangzhou city, China. Front. Psychiatry 13, 1018069 (2022).
Tung, T. H. & Hsiung, M. C. Work fatigue in a hospital setting: The experience at Cheng Hsin General hospital. Healthc. (Basel Switzerland) 9(6), 776 (2021).
Myers, J. A., Haney, M. F., Griffiths, R. F., Pierse, N. F. & Powell, D. M. Fatigue in air medical clinicians undertaking high-acuity patient transports. Prehospital Emerg. care 19 (1), 36–43 (2015).
Imani, F., Akhuleh, O. Z., Memarbashi, E. & Nasiri, E. Link between occupational fatigue and medical errors in surgical technologists. (2020).
Chen, J. Q. et al. The relationship between mindfulness, fatigue, and perceived symptoms among Frontline nurses who performed nucleic acid sample collection during the COVID-19 in China: A cross-sectional study. Psychol. Res. Behav. Manage. 16, 1165–1180 (2023).
Cunningham, T. R., Guerin, R. J., Ferguson, J. & Cavallari, J. Work-related fatigue: A hazard for workers experiencing disproportionate occupational risks. Am. J. Ind. Med. 65 (11), 913–925 (2022).
Juniartha, I. G. N., Sardjono, T. W. & Ningsih, D. K. A comparison of work-related fatigue and stress among emergency department nurses working in 7-7-10 and 12–12 shifts at the hospitals in Badung and Denpasar. Enfermería Clínica. 30, 74–77 (2020).
Manning, K., Zvolensky, M. J., Garey, L., Long, L. J. & Gallagher, M. W. The explanatory role of fatigue severity in the relation between COVID-19 perceived stress and depression, anxiety, and panic severity. Cogn. Behav. Ther. 51 (2), 89–99 (2022).
Wang, J. et al. The physical and mental health of the medical staff in Wuhan Huoshenshan Hospital during COVID-19 epidemic: A structural equation modeling approach. Eur. J. Integr. Med. 44, 101323 (2021).
Lu, Y. et al. Association of working hours and cumulative fatigue among Chinese primary health care professionals. Front. Public. Health 11, 1193942 (2023).
Silva-Costa, A., Rotenberg, L., Griep, R. H. & Fischer, F. M. Relationship between sleeping on the night shift and recovery from work among nursing workers: The influence of domestic work. J. Adv. Nurs. 67 (5), 972–981 (2011).
Li, M. et al. Associations of occupational stress, workplace violence, and organizational support on chronic fatigue syndrome among nurses. J. Adv. Nurs. 76 (5), 1151–1161 (2020).
Holmqvist, A., Berginström, N., Löfgren, M., Stålnacke, B. M. & Möller, M. C. Fatigue and cognitive fatigability in patients with chronic pain. Scand. J. Pain 24(1), 20230085 (2024).
Deng, G. et al. Linking doctor-patient relationship to medical residents’ work engagement: The influences of role overload and conflict avoidance. BMC Fam. Pract. 22 (1), 191 (2021).
Chalder, T. et al. Development of a fatigue scale. J. Psychosom. Res. 37 (2), 147–153 (1993).
Zhan, Y. et al. Factors associated with insomnia among Chinese front-line nurses fighting against COVID-19 in Wuhan: a cross-sectional survey. J. Nurs. Adm. Manag. 28 (7), 1525–1535 (2020).
Jing, M. J. et al. Reliability and construct validity of two versions of chalder fatigue scale among the general population in Mainland China. Int. J. Environ. Res. Public Health 13(1), 147 (2016).
Tie, H. et al. Symptom clusters and characteristics of cervical cancer patients receiving concurrent chemoradiotherapy: A cross-sectional study. Heliyon 9 (12), e22407 (2023).
Wu, J. et al. Subtypes of nurses’ mental workload and interaction patterns with fatigue and work engagement during coronavirus disease 2019 (COVID-19) outbreak: A latent class analysis. BMC Nurs. 20 (1), 206 (2021).
Cohen, S., Kamarck, T. & Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 24 (4), 385–396 (1983).
Cohen, S. & Williamson, G. M. Perceived stress in a probability sample of the United States: The social psychology of health: Claremont Symposium on Applied Social Psychology (1988).
Jiang, C. et al. The trends of psychosomatic symptoms and perceived stress among healthcare workers during the COVID-19 pandemic in China: Four cross-sectional nationwide surveys, 2020–2023. Psychiatry Res. 326, 115301 (2023).
Wang, Z. et al. Psychometric properties of the Chinese version of the perceived stress scale in policewomen. PloS One 6 (12), e28610 (2011).
Lu, W. et al. Chinese version of the perceived stress Scale-10: A psychometric study in Chinese university students. PloS One 12 (12), e0189543 (2017).
Bastien, C. H., Vallières, A. & Morin, C. M. Validation of the insomnia severity index as an outcome measure for insomnia research. Sleep Med. 2 (4), 297–307 (2001).
Morin, C. M., Belleville, G., Bélanger, L. & Ivers, H. The Insomnia severity index: Psychometric indicators to detect insomnia cases and evaluate treatment response. Sleep 34 (5), 601–608 (2011).
Yazdi, Z., Sadeghniiat-Haghighi, K., Zohal, M. A. & Elmizadeh, K. Validity and reliability of the Iranian version of the insomnia severity index. Malays. J. Med. Sci.: MJMS 19 (4), 31–36 (2012).
Castronovo, V. et al. Validation study of the Italian version of the Insomnia Severity Index (ISI). Neurol. Sci.: Off. J. Ital. Neurol. Soc. Ital. Soc. Clin. Neurophysiol. 37 (9), 1517–1524 (2016).
Wang, P. X., Wang, M. Z., Hu, G. X. & Wang, Z. M. Study on the relationship between workplace violence and work ability among health care professionals in Shangqiu City. Wei Sheng Yan jiu = J. Hygiene Res. 35 (4), 472–474 (2006).
Spitzer, R. L., Kroenke, K., Williams, J. B. & Löwe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 166 (10), 1092–1097 (2006).
Wu, F. et al. Association between intimate partner violence and prenatal anxiety and depression in pregnant women: A cross-sectional survey during the COVID-19 epidemic in Shenzhen, China. BMJ Open. 12 (5), e055333 (2022).
Martínez-Vázquez, S., Martínez-Galiano, J. M., Peinado-Molina, R. A., Gutiérrez-Sánchez, B. & Hernández-Martínez, A. Validation of general anxiety disorder (GAD-7) questionnaire in Spanish nursing students. PeerJ 10, e14296 (2022).
Kroenke, K., Spitzer, R. L. & Williams, J. B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 16 (9), 606–613 (2001).
Manea, L., Gilbody, S. & McMillan, D. A diagnostic meta-analysis of the patient health questionnaire-9 (PHQ-9) algorithm scoring method as a screen for depression. Gen. Hosp. Psychiatry 37 (1), 67–75 (2015).
Sun, L. et al. COVID-19 pandemic-related depression and anxiety under lockdown: the chain mediating effect of self-efficacy and perceived stress. Front. Psychiatry 14, 1100242 (2023).
Wang, W. et al. Reliability and validity of the Chinese version of the patient health questionnaire (PHQ-9) in the general population. Gen. Hosp. Psychiatry 36 (5), 539–544 (2014).
Smilkstein, G. The family APGAR: A proposal for a family function test and its use by physicians. J. Fam. Pract. 6 (6), 1231–1239 (1978).
Huang, J. et al. The relationship among pregnancy-related anxiety, perceived social support, family function and resilience in Chinese pregnant women: A structural equation modeling analysis. BMC Women’s Health 22 (1), 546 (2022).
Hahn, S. R., Thompson, K. S., Wills, T. A., Stern, V. & Budner, N. S. The difficult doctor-patient relationship: Somatization, personality and psychopathology. J. Clin. Epidemiol. 47 (6), 647–657 (1994).
Hahn, S. R. Physical symptoms and physician-experienced difficulty in the physician-patient relationship. Ann. Intern. Med. 134 (9 Pt 2), 897–904 (2001).
Du, J. et al. The validity and IRT psychometric analysis of Chinese version of difficult doctor-patient relationship questionnaire (DDPRQ-10). BMC Psychiatry 23 (1), 900 (2023).
Mathew, J. J., Joseph, M., Britto, M. & Joseph, B. Shift work disorder and its related factors among health-care workers in a tertiary care hospital in Bangalore, India. Pak. J. Med. Sci. 34 (5), 1076–1081 (2018).
Zhang, Y., Xu, Q., Ma, J., Wang, Z. & Lu, S. Pandemic fatigue and clinical front-line medical staff health, job status during the COVID-19 pandemic: A cross-sectional survey after the lifting of epidemic restrictions. Nurs. Open 11 (1), e2081 (2024).
Olude, O. A. et al. Mental health status of doctors and nurses in a Nigerian tertiary hospital: A COVID-19 experience. South. Afr. J. Psychiatry: SAJP : J. Soc. Psychiatrists South. Afr. 28, 1904 (2022).
Bensing, J. M., Hulsman, R. L. & Schreurs, K. M. Gender differences in fatigue: Biopsychosocial factors relating to fatigue in men and women. Med. Care. 37 (10), 1078–1083 (1999).
Williamson, R. J. et al. The relationship of fatigue to mental and physical health in a community sample. Soc. Psychiatry Psychiatr. Epidemiol. 40 (2), 126–132 (2005).
Wang, J. Effects of physical exercise motives on physical health and aerobic fitness of teenagers. Iran. J. Public. Health 50 (10), 2028–2037 (2021).
Jalilian, H., Shouroki, F. K., Azmoon, H., Rostamabadi, A. & Choobineh, A. Relationship between job stress and fatigue based on job demand-control-support model in Hospital nurses. Int. J. Prev. Med. 10, 56 (2019).
Harris, A. L., Carmona, N. E., Moss, T. G. & Carney, C. E. Testing the contiguity of the sleep and fatigue relationship: A daily diary study. Sleep. 44(5), zsaa252 (2021).
Kredlow, M. A., Capozzoli, M. C., Hearon, B. A., Calkins, A. W. & Otto, M. W. The effects of physical activity on sleep: A meta-analytic review. J. Behav. Med. 38 (3), 427–449 (2015).
Korompeli, A., Chara, T., Chrysoula, L. & Sourtzi, P. Sleep disturbance in nursing personnel working shifts. Nurs. Forum 48 (1), 45–53 (2013).
Alimoradi, Z. et al. Effects of cognitive behavioral therapy for insomnia (CBT-I) on quality of life: A systematic review and meta-analysis. Sleep Med. Rev. 64, 101646 (2022).
Bunevicius, A., Stankus, A., Brozaitiene, J., Girdler, S. S. & Bunevicius, R. Relationship of fatigue and exercise capacity with emotional and physical state in patients with coronary artery disease admitted for rehabilitation program. Am. Heart J. 162 (2), 310–316 (2011).
Harbishettar, V., Krishna, K. R., Srinivasa, P. & Gowda, M. The enigma of doctor-patient relationship. Indian J. Psychiatry 61 (Suppl 4), S776–s81 (2019).
Xie, Z., Qiu, Z. Q. & Zhang, T. H. [Influence of patients’ attitude on doctors’ satisfaction with the doctor-patient relationship]. Beijing Da Xue Xue bao Yi xue ban = J. Peking Univ. Health Sci. 41 (2), 141–143 (2009).
Kumar, B., Paul, U. K. & Pal, D. K. Perception of doctor-patient relationship in the present time from the viewpoint of doctors: A qualitative study at a tertiary health-care center in eastern India. Indian J. Commun. Med.: Off. Publ. Indian Assoc. Prev. Soc. Med. 45 (1), 100–103 (2020).
Sommer, A., Grothus, S., Claus, B. B., Stahlschmidt, L. & Wager, J. Fatigue in children and adolescents: A population-based longitudinal study on fatigue and chronic pain. J. Pediatr. Psychol. 48 (7), 626–635 (2023).
Sunwoo, J. S., Kim, D., Chu, M. K., Yun, C. H. & Yang, K. I. Fatigue is associated with depression independent of excessive daytime sleepiness in the general population. Sleep. Breath. = Schlaf Atmung. 26 (2), 933–940 (2022).
Wong, L. R., Flynn-Evans, E. & Ruskin, K. J. Fatigue risk management: the impact of Anesthesiology residents’ work schedules on job performance and a review of potential countermeasures. Anesth. Analg. 126 (4), 1340–1348 (2018).
Acknowledgements
We would like to thank all the doctors and nurses who took time out of their busy schedules to participate in this study.
Funding
This study had no funding support.
Author information
Authors and Affiliations
Contributions
BW, XC, SRH, and YW conducted the study conception and design. BW, DML, SRH, and YW collected the data. BW, WSY, and DW analyzed the data and drafted and revised the manuscript. All authors contributed to the manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Wang, B., Yang, W., Wang, Y. et al. Current situation and related factors of fatigue among doctors and nurses in tertiary general hospitals in Northeast China. Sci Rep 15, 9548 (2025). https://doi.org/10.1038/s41598-025-87400-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-025-87400-1
