
Abstract
Sustentacular fragment displacement is not uncommon in calcaneal fractures. The factors that suggest a possible displacement of sustentacular fragment are still unclear. Displaced intra-articular calcaneal fractures with calcaneocuboid joint involvement are the most common type of calcaneal fracture. The purpose of this study is to investigate whether there is a correlation between calcaneocuboid joint involvement and sustentacular fragment displacement in displaced intra-articular calcaneal fractures. We collected basic data and CT scans of male patients with displaced intra-articular calcaneal fractures who were hospitalized in the north district of our hospital from July 2021 to June 2024. Three different logistic regression models were employed to analyze the relationship between calcaneocuboid joint involvement and sustentacular fragment displacement. Additionally, stratification analyses and their interactions were further carried out. 144 calcaneal fractures in 131 male patients were included in our study. 63 cases, accounting for 43.75%, exhibited sustentacular fragment displacement. In logistic regression analysis, a favorable association was noted between calcaneocuboid joint involvement and sustentacular fragment displacement (OR = 2.33, 95% CI: 1.18–4.59, P < 0.05). In model 2, the association retained statistical significance after adjusting for confounding factor (OR = 2.27, 95% CI: 1.15–4.51, P < 0.05). In model 3, further adjustment for all potential confounding factors also showed a statistically significant association (OR = 2.31, 95% CI: 1.14–4.68, P < 0.05).Similar results were obtained in stratified analyses. Among male patients with displaced intra-articular calcaneal fractures, it was initially discovered that calcaneocuboid joint involvement can significantly increase the risk of sustentacular fragment displacement, particularly in Sanders type 3 and 4 fractures and when the proportion of the posterior facet in sustentacular fragment is less than 50%.
Similar content being viewed by others

Introduction
Calcaneal fractures, the most common type of tarsal bone fractures, account for 1.2% of all fractures and are more frequently observed in men1,2. The injury mechanism is typically due to falling from a height or being involved in a traffic accident2,3,4. Over 70% of calcaneal fractures are intra-articular, and 95% of these intra-articular fractures result in displacement5. Most displaced intra-articular calcaneal fractures require surgical treatment to achieve better function6,7. The extended lateral approach and the sinus tarsi approach are commonly used surgical exposures8,9. Traditionally, the sustentacular fragment has been considered stable and used as a reference point for reduction during surgery10,11,12,13. However, in 2013, Berberian first reported that sustentacular fragment is not constant and can undergo both translation and angular displacement, with a total displacement rate of 42%. Furthermore, the incidence of displacement tends to increase with higher Sanders classification grades14.Subsequent research has also confirmed the correlation between the Sanders classification and sustentacular fragment displacement15. Some scholars have reported that the width of the sustentacular fragment is correlated with the stability of the sustentaculum tali16,17. Apart from the above two factors, no other risk factors of sustentacular fragment displacement have been identified.
In 1993, Zwipp introduced a new classification system for calcaneal fractures, emphasizing the importance of the medial column (sustentaculum tali) and the lateral column (calcaneocuboid joint)18. Rammelt stated that in calcaneal fractures, the restoration of the medial and lateral columns is essential to reestablish the biomechanical integrity of the hindfoot19. Displaced intra-articular calcaneal fractures with calcaneocuboid joint involvement are the most common type of calcaneal fracture, compared to those with sustentacular fragment displacement5. Reports have found that in displaced calcaneal fractures, about three-fifths involve the calcaneocuboid joint and this may also be correlated with the Sanders classification5,20,21.
Given the high prevalence of sustentacular fragment displacement and calcaneocuboid joint involvement, their shared risk factors, and their critical roles in calcaneal fractures, there is an urgent need to investigate the potential correlation between them. To date, no research has been conducted on the correlation between calcaneocuboid joint involvement and sustentacular fragment displacement in calcaneal fractures. The primary objective of this study is to explore whether calcaneocuboid joint involvement increases the risk of sustentacular fragment displacement in male patients with displaced intra-articular calcaneal fractures.
Materials and methods
After obtaining approval from the Clinical Trial Ethics Committee of Yantaishan Hospital, we conducted a retrospective analysis using continuous sampling of patients with calcaneal fractures admitted to the Northern District of our hospital between July 2021 and June 2024. The inclusion criteria were as follows: (1) The fracture line involves the posterior subtalar joint surface and is displaced; (2) CT scan was performed at our hospital; (3) The patient is male. The exclusion criteria included: (1) Extra-articular calcaneal fracture; (2) The fracture line involves the posterior subtalar joint surface but is not displaced; (3) No CT data available; (4) Female. A step-off of ≥ 2 mm in the articular surface on CT imaging is defined as fracture displacement. Basic information collected includes: age, underlying diseases, side of injury, presence of bilateral injuries, occurrence and details of multiple injuries. Voluntary informed consent was obtained in writing from participants prior to the study. And the study was conducted in accordance with ethical standards laid down in an appropriate version of the Declaration of Helsinki.
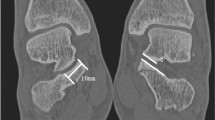
The measurement and recording of CT data were each completed by two trauma surgeons. Using CT cross-sectional and sagittal images, the involvement of calcaneocuboid joint and the middle subtalar joint was assessed. Oblique coronal CT images, perpendicular to the posterior facet of the subtalar joint, were used to classify all calcaneal fractures according to the Sanders classification system. Additionally, it was recorded whether the proportion of the posterior facet of sustentacular fragment was greater than 50%. The oblique coronal plane of the calcaneus was adjusted to be perpendicular to the middle subtalar joint surface of the calcaneus, and the translation and angular displacement of the sustentacular fragment at the midpoint of the middle subtalar joint surface were measured. It is shown in Fig. 1. A displacement of more than 2 mm or an angulation greater than 5° was set as indicative of sustentacular fragment displacement.

(A) Non-displaced sustentacular fragment in calcaneus fracture. (B) Transverse displaced sustentacular fragment in calcaneus fracture. (C) Angular displaced sustentacular fragment in calcaneus fracture.
Data are presented as frequencies (percentages) for categorical variables according to whether sustentacular fragment displacement occurs. In an effort to assess the correlation between calcaneocuboid joint involvement and sustentacular fragment displacement, we employed logistic regression models. Model 1 was an unadjusted model with no additional variables taken into account. Model 2 incorporated adjustments for confounder including proportion of posterior facet in sustentacular fragment only. We selected confounders due to their correlation with the desired outcomes or a variation in the effect size greater than 10%. Model 3 was adjusted for suspected factors, including age, side of injury, multiple trauma, proportion of posterior facet in sustentacular fragment, middle subtalar facet fracture and Sanders classification. To further evaluate the potential influence of different populations, stratification and interaction analyses were further performed based on the following variables: age (< 50 vs. ≥ 50 years), which foot (left/right), multiple trauma (yes/no), middle subtalar facet fracture (yes/no), Sanders classification (type II vs. III/iV), and proportion of posterior facet in sustentacular fragment (> 50% vs. < 50%).
Statistical analyses were performed using R statistics packages (available at http://www.r-project.org, courtesy of The R Foundation) and EmpowerStats (accessible at http://www.empowerstats.com, provided by X&Y Solutions, Inc., Boston, MA). Statistical significance was established at a P value threshold of less than 0.05 (two-tailed test).
Results
144 calcaneus fractures in 131 male patients were included in the study. The average age of the patients was 49 years (range from 16 to 74 years). Among these, 14 cases had underlying diseases (hypertension alone in 10 cases, diabetes alone in 3 cases, and both conditions in 1 case). There were 67 cases on the left side and 77 cases on the right side. 74 cases were accompanied by multiple injuries, of which 79.9% were accompanied by foot fractures, including 40 cases of bilateral calcaneal fractures. Tibial and fibula fractures and spinal fractures accounted for 20.3% and 17.6%, respectively. Less common multiple injuries included femoral fractures, rib fractures, pelvic fractures, and upper limb fractures. Details of multiple injuries are shown in Table 1.
All cases were classified according to the Sanders classification system, with 30 cases of type IIA, 65 cases of type IIB, 18 cases of type IIC, 10 cases of type IIIAB, 9 cases of type IIIAC, 9 cases of type IIIBC, and 3 cases of type IV. In 70 cases, the posterior facet of the sustentacular fragment accounted for less than 50% of the facet. The fracture line involved the calcaneocuboid joint in 77 cases and the middle subtalar joint facet in 48 cases. Table 2 provides an overview of the population characteristics categorized by whether the sustentacular fragment was displaced.
A total of 63 cases, accounting for 43.75%, exhibited sustentacular fragment displacement, with transverse displacement making up 90.48% and an average displacement of 3.25 mm. Angular displacement was observed in 22.22% of the cases, with an average angulation of 8.09°. For more details, refer to Table 3.
Univariate analysis revealed that, compared to the group without calcaneocuboid joint involvement, the group with calcaneocuboid joint involvement had a 133% increased risk of sustentaculum tali fragment displacement (95% CI: 1.18–4.59; p < 0.01). Additionally, age, underlying health conditions, which foot, multiple injuries, middle subtalar facet fracture, proportion of the posterior facet in sustentacular fragment, and Sanders classification were positively associated with sustentacular fragment displacement, though all with p-values < 0.05. Details are shown in Table 4.
To investigate the association between calcaneocuboid joint involvement and sustentacular fragment displacement, we performed a logistic regression analysis. In Model 1, unadjusted for any covariates, calcaneocuboid joint involvement was associated with a 133% increase in the risk of sustentacular fragment displacement (95% CI, 1.18 to 4.59). In Model 2, after adjustment for confounding factor, the proportion of posterior facet involvement in the sustentacular fragment, the risk increased by 127% (95% CI, 1.15 to 4.51). In Model 3, further adjustment for almost all covariates, such as proportion of posterior facet in sustentacular fragment, Sanders classification, multiple injuries, middle subtalar facet fracture, age and injury laterality, resulted in a 131% increase in risk (95% CI,1.14 to 4.68). Details are shown in Table 5.
We performed stratified analyses on age, the side of injury, multiple injuries, middle subtalar facet fracture, Sanders classification and proportion of posterior facet in sustentacular fragment, while also conducting interaction tests. In stratified analysis, adjust for the proportion of posterior facet in sustentacular fragment. When layered by this factor, no confounding factors require adjustment. In the age group of 50 and above, calcaneocuboid joint involvement led to a 165% increase in the risk of sustentacular fragment displacement (95% CI, 0.98 to 7.11), whereas in the under-50 age group, the risk was elevated by 85% (95% CI, 0.69 to 4.98). For injuries on the right side, the risk associated with calcaneocuboid joint involvement rose by 161% (95% CI, 0.98 to 6.94), and for the left side, the risk increased by 84% (95% CI, 0.68 to 4.96). In individuals without multiple injuries, this risk increased by 188% (95% CI, 0.98 to 8.43) due to calcaneocuboid joint involvement, and in those with multiple injuries, the risk was raised by 95% (95% CI, 0.77 to 4.93). When the middle subtalar facet was fractured, the engagement of calcaneocuboid joint resulted in an increased risk of 186% (95% CI, 0.84 to 9.71); conversely, in the absence of such a fracture, the risk grew by 104% (95% CI, 0.89 to 4.69). All interaction test results within these groups were statistically non-significant.
In the subset where the posterior facet of the sustentacular fragment occupied less than 50%, calcaneocuboid joint involvement was associated with a 385% increase in the risk of sustentacular fragment displacement (95% CI, 1.74 to 13.49). By contrast, in the other group, the risk increased by 12% (95% CI, 0.44 to 2.90). Within the Sanders classification, calcaneocuboid joint involvement was associated with a 980% increase in the risk of sustentacular fragment displacement in types III and IV (95% CI, 1.69 to 68.94), while the risk increased by 62% in type II (95% CI, 0.76 to 3.47). The p-value for interaction in both stratified analyses mentioned above was less than 0.05. Details are shown in Fig. 2.

Stratified analysis of the relationship between sustentacular fragment displacement and calcaneocuboid joint involvement.
Discussion
Calcaneal fractures are relatively common among foot fractures, often resulting from vertical force impacts, which can lead to one or more sites of fracture1,2,3,4. Mitchell found that over 75% of calcaneal fractures were isolated injuries. The most common concomitant fractures were lower extremity fractures, accounting for 13.2% of the total, followed by spinal fractures at 6.3%. Bilateral calcaneal fractures occurred in 55 individuals, representing only 7.9%3. A study involving 5,977 patients with calcaneal fractures found that 68% of the patients had isolated calcaneal fractures. Common concomitant fractures were, in descending order: spinal fractures at 8%, ankle fractures at 8%, distal radius fractures at 4%, and talar fractures at 3%22. In contrast, our study found that isolated calcaneus fractures accounted for only 48.6%. The most common concomitant fracture was foot fracture, with a total of 59 cases. This included 40 bilateral calcaneus fractures in 27 patients, accounting for as high as 20.6% of all patients. The remaining concomitant fractures were, in order: tibial and fibular, spinal, rib, and femur fractures, with only 1 upper limb fracture.
Due to the numerous ligamentous structures connected to the sustentaculum tali, it was previously considered constant in calcaneal fractures13,15,23,24. In a study of 25 calcaneal fractures, Heger found that 72% of the cases exhibited sustentacular fragment displacement25. However, Gilmer challenged the finding through a study of 32 calcaneal fractures and insisted that sustentacular fragment does not undergo displacement23. In 2013, Berberian conducted the first detailed study on whether sustentacular fragment is constant, including a total of 100 calcaneal fractures, and found that 42% had sustentacular fragment displacement, of which 25% were angular displacement and 24% were transverse displacement14. In 2014, Gitajn found through a study of 212 calcaneal fractures that 20.3% had sustentacular fragment displacement15. Shi collected 81 cases of intra-articular calcaneal fractures, of which 6 cases (28.6%) had sustentacular fragment displacement, with Sanders type 4 fractures accounting for 83.3%26. We also found that sustentacular fragment displacement in calcaneal fractures is not uncommon, accounting for 43.75%. However, the most common type was transverse displacement, which accounted for 90.48%, while angular displacement only accounted for 22.22%. Studies mentioned above have different definitions of sustentacular fragment displacement14,15,26. Perhaps we need to standardize the definition of sustentacular fragment displacement to facilitate subsequent related research.
Our analysis demonstrates that 53.5% of displaced intra-articular calcaneal fractures involve the calcaneocuboid joint, which is slightly lower than findings from comparable studies. For instance, Vosoughi et al., in a CT-based study of 957 calcaneal fractures, reported calcaneocuboid joint involvement in 59.9% of intra-articular cases5. Kinner reported a 68% rate of calcaneocuboid joint involvement in intra-articular subtalar calcaneal fractures27. Studies by Miric and Patterson in 1998 and Zwipp et al. in 2004 reported that the incidence of calcaneocuboid joint involvement in displaced intra-articular calcaneal fractures is about 60%20,21. As the Sanders classification level increases, calcaneocuboid joint involvement becomes more common5,20.
Currently, no studies have investigated whether there is a correlation between calcaneocuboid joint involvement and sustentacular fragment displacement. Through this study, we found for the first time that in male patients with displaced intra-articular calcaneal fractures, calcaneocuboid joint involvement more than doubles the risk of sustentacular fragment displacement. It has been reported that fractures involving > 50% of the posterior facet carried a 128% increased risk for sustentacular fragment displacement, and three-part or four-part fractures carried a 155% increased risk for sustentacular fragment displacement14. Therefore, we conducted a stratified analysis based on the proportion of the posterior facet in the sustentacular fragment and the Sanders classification. When the proportion of the posterior facet in the sustentacular fragment is less than 50%, calcaneocuboid joint involvement increases the risk of sustentacular fragment displacement by 385%. In groups with Sanders type III and above, the risk even increases by 980%. This indicates that as the proportion of the posterior facet in the sustentacular fragment decreases and the Sanders classification level increases, there is a strong correlation between calcaneocuboid joint involvement and sustentacular fragment displacement.
The sustentacular fragment displacement is more common in right calcaneal fractures, consistent with previous studies. Furthermore, we found that in right-sided calcaneal fractures, the risk of sustentacular fragment displacement is higher when the calcaneocuboid joint is involved compared to left-sided calcaneal fractures. In the stratified analysis by age, the risk of sustentacular fragment displacement was higher in the group aged 50 years and older compared to the group younger than 50 years. This may indicate that as age increases, the risk of sustentacular fragment displacement with calcaneocuboid joint involvement also increases.
Our study has several limitations. Firstly, the cross-sectional research approach only allows for the evaluation of correlations and does not provide data on the chronological linkage between cause and effect. Secondly, despite efforts to adjust for known confounding factors, there is still the possibility of overlooked or unaccounted confounders that may impact the findings. Lastly, in subgroup analysis, a small sample size, such as only 31 cases in Sanders type 3 and 4, can lead to overly broad confidence intervals and estimation bias. Increasing the sample size is necessary to enhance statistical power.
This is a large scale study of sustentacular fragment displacement in calcaneal fractures to date. By analyzing 144 displaced intra-articular calcaneal fractures in males, the study confirmed that sustentacular fragment displacement is not uncommon in calcaneal fractures. Additionally, it was discovered for the first time that calcaneocuboid joint involvement significantly increases the risk of sustentacular fragment displacement, particularly in Sanders type 3 and 4 fractures and when the proportion of the posterior facet in the sustentacular fragment is less than 50%.
Data availability
Data generated and analyzed is provided within the supplementary information files.
References
Court-Brown, C. M. & Caesar, B. Epidemiology of adult fractures: A review. Injury 37, 691–697 (2006).
Bohl, D. D. et al. Demographics, mechanisms of injury, and concurrent injuries associated with calcaneus fractures: A study of 14 516 patients in the American college of surgeons National trauma data bank. Foot Ankle Spec. 10, 402–410 (2017). Demographics.
Mitchell, M. J., McKinley, J. C. & Robinson, C. M. The epidemiology of calcaneal fractures. Foot 19, 197–200 (2009).
Humphrey, J. A., Woods, A. & Robinson, A. H. N. The epidemiology and trends in the surgical management of calcaneal fractures in England between 2000 and 2017. Bone Jt. J. 101-B, 140–146 (2019).
Vosoughi, A. R. et al. Different types and epidemiological patterns of calcaneal fractures based on reviewing CT images of 957 fractures. Foot Ankle Surg. 28, 88–92 (2022).
Schleunes, S., Lobos, E. & Saltrick, K. Current management of Intra-Articular calcaneal fractures. Clin. Podiatr. Med. Surg. 41, 473–490 (2024).
Salameh, M. et al. Management of displaced intra-articular calcaneal fractures; current concept review and treatment algorithm. Eur. J. Orthop. Surg. Traumatol. 33, 779–785 (2022).
Rammelt, S. & Swords, M. P. Calcaneal fracture?s—Which approach for which fracture?? Orthop. Clin. N. Am. 52, 433–450 (2021).
Khazen, G. & Rassi, C. K. Sinus Tarsi approach for calcaneal fractures. Foot Ankle Clin. 25, 667–681 (2020).
Stephenson, J. R. Displaced fractures of the Os Calcis involving the subtalar joint: the key role of the superomedial fragment. Foot Ankle. 4, 91–101 (1983).
Stephenson, J. R. Treatment of displaced intra-articular fractures of the calcaneus using medial and lateral approaches, internal fixation, and early motion. J. Bone Jt. Surg. 69, 115–130 (1987).
Burdeaux, B. D. The medical approach for calcaneal fractures. Clin. Orthop. Relat. Res. 96–107 (1993).
Keener, B. J. & Sizensky, J. A. The anatomy of the calcaneus and surrounding structures. Foot Ankle Clin. 10, 413–424 (2005).
Berberian, W. et al. Displacement of the sustentacular fragment in Intra-Articular calcaneal fractures. J. Bone Jt. Surg. 95, 995–1000 (2013).
Gitajn, I. L. et al. Anatomic alignment and integrity of the sustentaculum Tali in Intra-Articular calcaneal fractures. J. Bone Jt. Surg. 96, 1000–1005 (2014).
Yan, H., Na, H. D., Park, J. J. & Park, C. H. Study on sustentaculum Tali fragment constancy in intraarticular calcaneus fracture. J. Orthop. Trauma 37, e422–e427 (2023).
Park, C. H., Choi, H. & Park, J. Factors related to the inconstancy of sustentaculum Tali fragments in Intra-Articular calcaneus fractures. Foot Ankle Orthop. 7 (2022).
P8472474_14999866.pdf.
Rammelt, S. & Zwipp, H. Fractures of the Calcaneus: current treatment strategies. Acta Chir. Orthop. Traumatol. Cech 81, 177–196 (2014).
Miric, A. & Patterson, B. M. Pathoanatomy of intra-articular fractures of the calcaneus. J. Bone Jt. Surg. Am. 80, 207–212 (1998).
Zwipp, H., Rammelt, S. & Barthel, S. Calcaneal fractures—open reduction and internal fixation (ORIF). Injury 35, 46–54 (2004).
Haapasalo, H. et al. Epidemiology of calcaneal fractures in Finland. Foot Ankle Surg. 23, 321–324 (2017).
Gilmer, P. W. et al. Computerized tomographic analysis of acute calcaneal fractures. Foot Ankle 6, 184–193 (1986).
Smitaman, E. & Davis, M. Hindfoot fractures: injury patterns and relevant imaging findings. RadioGraphics 42, 661–682 (2022).
Heger, L., Wulff, K. & Seddiqi, M. S. Computed tomography of calcaneal fractures. Am. J. Roentgenol. 145, 131–137 (1985).
Shi, G., Lin, Z., Liao, X., Liu, W. & Cai, X. Two and three-dimensional CT mapping of the sustentacular fragment in intra-articular calcaneal fractures. Sci. Rep. 12 (2022).
Kinner, B., Schieder, S., Müller, F., Pannek, A. & Roll, C. Calcaneocuboid joint involvement in calcaneal fractures. J. Trauma 68, 1192–1199 (2010).
Acknowledgements
The authors gratefully acknowledge the help and guidance provided by their academic and research teams. This study was conducted without any financial support.
Author information
Authors and Affiliations
Contributions
Wenchuang Fan and Chuanqiang Jiang designed the study. Haining Zuo, Xing Lu, Xinglin Zhang and Zhiyong Zhou performed data collection. Wenchuang Fan performed statistical analysis and drafed the manuscript. Chuanqiang Jiang revised the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Fan, W., Zuo, H., Lu, X. et al. The correlation between calcaneocuboid joint involvement and sustentacular fragment displacement among male patients with displaced intra-articular calcaneal fractures. Sci Rep 15, 8367 (2025). https://doi.org/10.1038/s41598-025-92639-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-025-92639-9
