
Abstract
Functional constipation is a common gastrointestinal disorder influenced by dietary, anthropometric, and demographic factors. However, the combined impact of these factors on constipation symptoms remains underexplored, particularly within the Peruvian population. To assess the association of nutritional knowledge, fiber-rich food consumption, body mass index (BMI), and sex with functional constipation symptoms in Peruvian adults. A cross-sectional study was conducted among 404 Peruvian adults selected through non-probability sampling. Nutritional knowledge (assessed using the Dietary Fiber Habits and Knowledge Questionnaire), fiber-rich food consumption (measured with the Block Instrument), BMI (self-reported and calculated), and constipation symptoms (evaluated using the Rome III International Diagnostic Questionnaire) were analyzed. Hierarchical regression analysis was performed to evaluate the impact of the variables on constipation symptoms. The hierarchical regression analysis, conducted in four blocks, demonstrated a progressive increase in the explained variance. In the fourth block, nutritional knowledge (β = − 0.173, p = 0.006, CI [− 0.296, − 0.050]) and consumption of high-fiber foods (β = − 0.227, p < 0.001, CI [− 0.351, − 0.103]) were associated with a reduction in constipation symptoms, while BMI (β = 0.230, p < 0.001, CI [0.108, 0.353]) and being female (β = 0.153, p = 0.014, CI [0.031, 0.274]) were associated with an increase in symptoms. The final model accounted for 16.4% of the total variance (adjusted R2 = 0.164), with fiber consumption contributing to a 5.2% increase in explained variance (∆R2 = 0.052). These findings underscore the importance of implementing public health educational and dietary strategies to address constipation through preventive and personalized approaches.
Similar content being viewed by others

Introduction
Constipation is a gastrointestinal disorder defined by difficulty or infrequent bowel movements, often accompanied by hard stools or a sensation of incomplete evacuation1. This condition affects a significant portion of the global population, with prevalence estimates ranging widely from 1 to 80% depending on the criteria used for diagnosis2,3. In Latin America, the prevalence ranges from 15 to 30%4. In Peru, although specific studies are limited, available research indicates a prevalence of approximately 20%, particularly among adults and urban populations5. This highlights the need for further research to better understand the factors contributing to constipation in the Peruvian context. Additionally, constipation disproportionately affects children, with up to 37% experiencing this condition, accounting for 90–95% of intestinal issues in this population5.
Constipation is often closely linked to dietary and lifestyle factors, including insufficient fiber intake and a high BMI6,7. Furthermore, this condition impacts not only physical health but also emotional well-being and overall quality of life8. In the social sphere, constipation represents a significant burden for individuals and healthcare systems, contributing to work absenteeism, frequent medical consultations, and excessive use of laxatives, which may result in long-term complications9. Therefore, identifying the predisposing factors for this disorder can serve as a foundation for developing effective and targeted interventions tailored to the Peruvian population.
Nutritional knowledge
Nutritional knowledge, defined as the ability to recognize and apply principles of a balanced diet, has been identified as a crucial factor in promoting healthy eating behaviors10. To date, no studies have specifically examined the influence of nutritional knowledge on the occurrence or management of constipation. However, the role of nutritional knowledge as a determinant of eating habits suggests its potential relevance in this relationship. Evidence indicates that greater awareness of nutritional needs may encourage the adoption of dietary practices that support bowel health11. For instance, higher levels of nutritional knowledge are associated with increased consumption of fiber-rich foods, such as fruits, vegetables, and whole grains, which are essential for the prevention and management of constipation12.
On the other hand, previous research has emphasized that a lack of knowledge about dietary fiber sources and its role in digestive function can contribute to insufficient fiber intake, potentially exacerbating constipation symptoms13. In populations with low levels of nutritional education, a higher prevalence of gastrointestinal problems has been observed, supporting the hypothesis that nutritional education could be an effective strategy for preventing these conditions14. Although research on the relationship between nutritional knowledge and constipation is limited, studies on dietary education in other areas of bowel health suggest that targeted educational interventions could positively impact the reduction of constipation symptoms15,16. Intervention programs that encourage adequate fiber and fluid intake, grounded in a stronger understanding of basic nutrition principles, have demonstrated promising results in improving dietary habits and digestive health17,18,19.
Fiber intake
Dietary fiber plays a fundamental role in the prevention and management of constipation, as it contributes to the increase of stool volume and softness, facilitating intestinal transit20. Soluble fiber, found in foods such as fruits, oats, and legumes, forms a gel-like substance in the digestive tract that enhances stool consistency and facilitates its passage through the colon21. On the other hand, insoluble fiber, present in foods such as whole grains and vegetables, increases fecal volume and stimulates peristaltic movement21. The recommended daily fiber intake for adults ranges from 18 to 38 g, equivalent to approximately 8–20 g per 1000 kcal consumed22. The World Health Organization (WHO)/Food and Agriculture Organization (FAO) and the European Food Safety Authority (EFSA) recommend an average daily intake of 25 g of fiber for adults. However, most individuals consume less than half of this recommended amount22,23. At the national level, it has been observed that the Peruvian population tends to follow diets low in fiber, with daily consumption falling below the recommended levels24. This is partly attributed to a preference for processed foods and a lack of awareness about the benefits of fiber-rich foods24.
Numerous studies have demonstrated that dietary habits play a significant role in the onset and management of functional constipation21,25. A systematic review by Yang et al.26 highlighted that low fiber intake is one of the most common factors associated with functional constipation and that increasing fiber intake significantly alleviates symptoms in patients across various age groups. This finding is corroborated by other studies21,25, which conclude that fiber supplementation can shorten the duration of constipation episodes and increase stool frequency by adding bulk to the stool. This facilitates its passage through the digestive system and is widely regarded as a primary treatment for constipation. In the Peruvian context, some studies have observed an association between the consumption of foods rich in fiber and the presence of constipation. For example, a study conducted with a group of children, found a statistically significant relationship between fiber intake and the occurrence of constipation27. Another study conducted in the hospital setting has confirmed these statistically significant correlations between low dietary fiber intake and constipation (p < 0.001)28. However, studies conducted on healthy young adults remain scarce.
Elevated BMI
Obesity is an escalating public health problem worldwide, with its prevalence having tripled since 197529. In Peru, the National Health Survey indicates that obesity affects 26.3% of the adult population in urban areas and 14% in rural areas, reflecting a concerning scenario where sedentary lifestyles and diets high in processed foods are increasingly prevalent30. BMI, a key indicator of obesity, has been recognized as a factor that may contribute to the occurrence of functional constipation25. This relationship can be explained by two main mechanisms. First, a high BMI is often associated with a sedentary lifestyle, which reduces intestinal motility and promotes the development of functional constipation31. Second, the accumulation of adipose tissue may contribute to chronic low-grade inflammation, negatively impacting neurogastrointestinal function and disrupting intestinal transit32. Therefore, it is crucial to address obesity as a key factor in the prevention and management strategies for functional constipation.
A recent study demonstrated that a higher BMI, specifically values above 28 kg/m2, is associated with an increased risk of constipation. Similarly, other indicators of obesity, such as a waist-to-height ratio ranging from 58.3 to 64.8 and a lipid accumulation product index between 50.8 and 90.1, also exhibited a positive correlation with constipation33. Interestingly, the study found that a higher weight-adjusted waist circumference index (WWI) was associated with a lower risk of constipation, even after adjusting for various confounding variables33. On the other hand, a study involving 10,000 Japanese participants revealed that men with constipation tended to have a significantly lower BMI compared to those without constipation34. Moreover, this study found a significant relationship between BMI and educational level: individuals with only lower secondary education had the highest BMI, followed by those who had completed upper secondary education. However, a population-based study involving 14,238 adults revealed a nonlinear relationship between WWI and chronic constipation, identifying a cutoff point of 9.77. To the left of this cutoff, an increase in WWI was associated with a higher risk of constipation, while no statistically significant association was observed to the right of the cutoff point35. Nevertheless, it is essential to monitor central obesity using indicators such as the weight-adjusted waist index in the context of bowel health. Maintaining healthy levels of body fat is crucial to promoting regular bowel habits and preventing gastrointestinal disorders such as constipation.
Sex
Constipation is a multifactorial disorder influenced by a range of biological, sociodemographic, and lifestyle factors. Among these, sex has emerged as a critical variable for understanding differences in the prevalence, characteristics, and impact of constipation across various population groups36. Recent studies have demonstrated not only a higher prevalence of constipation among women but also notable differences in perception, symptom patterns, and the functional impact of this condition37,38,39.
Numerous studies have provided relevant findings highlighting the particularities of constipation from a sex-difference perspective. Specifically, multiple studies have consistently shown that women report a significantly higher prevalence of constipation compared to men. A Brazilian study revealed that 37.2% of women reported experiencing constipation, compared to only 10.2% of men38. Another similar study confirmed this trend, reporting that women were 2.5 times more likely to experience constipation than men40. These differences may be attributed to biological, hormonal, and cultural factors that influence bowel motility and habits. Furthermore, a Japanese study found that 37.5% of women perceived themselves as constipated, compared to 19.1% of men, highlighting not only the higher prevalence among women but also a greater self-awareness or perception of the condition39. This is consistent with research emphasizing how hormonal factors, such as fluctuations in estrogen and progesterone during the menstrual cycle, pregnancy, and menopause, impact bowel motility and may contribute to the development of constipation in women36.
On the other hand, sex differences in constipation extend beyond prevalence to include its functional impact on quality of life. One study found that women with constipation experienced greater limitations in areas such as mobility, self-care, and social participation compared to women without constipation37. These findings underscore the importance of considering sex as a key variable in the study of constipation, as women not only exhibit a higher prevalence of the condition but also experience greater impacts on their physical and social well-being.
The current study
Despite the numerous studies examining factors associated with constipation, significant gaps remain in the literature regarding the direct relationship between nutritional knowledge and this gastrointestinal disorder. While research indicates that greater nutritional knowledge can improve eating habits by promoting adequate fiber and fluid intake, its specific impact on the prevalence and management of functional constipation remains poorly understood. The limited research on this topic highlights the need to explore the role of nutrition education as a key tool for promoting intestinal health, particularly in contexts where the prevalence of constipation is high.
In Peru, research on the association between factors such as nutritional knowledge, high-fiber food consumption, BMI, and constipation remains limited. This knowledge gap highlights the importance of a comprehensive analysis of these elements within the local context, taking into account the specific characteristics of the Peruvian population. Understanding these interactions could be pivotal in developing more effective prevention and intervention strategies to improve digestive health and, consequently, individuals’ quality of life. This study aims to address these gaps in the literature by examining how these factors are associated with constipation symptoms in Peruvian adults. The findings will provide a deeper understanding of the mechanisms linking these factors to bowel health and support the development of educational strategies and preventive interventions tailored to the local context. This is particularly important for informing public policies and health promotion programs in Peru. Accordingly, this study examines how nutritional knowledge, frequency of fiber-rich food consumption, and BMI are associated with functional constipation symptoms in Peruvian adults.
Materials and methods
Design and participants
A cross-sectional was carried out41. The independent variables in this study were nutritional knowledge, consumption of fiber-rich foods, and BMI, while the dependent variable was constipation symptoms.
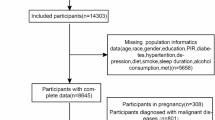
The sample consisted of 404 Peruvian adults, both men and women, aged 18 to 59 years, selected through non-probabilistic purposive sampling. Participants were included if they met the eligibility criteria, which included not having diagnosed with gastrointestinal diseases, not being under treatment with medications that affect intestinal function, and being willing to complete the study questionnaires. Individuals with medical conditions that could interfere with the assessment of constipation symptoms or with limitations in adequately completing the questionnaire were excluded. Data collection took place between October and November 2024 using a structured questionnaire. Social media platforms such as Facebook were utilized for distribution, and responses were recorded via the Microsoft Forms platform, facilitating access and participation.
Using the statistical program G*Power 3.1.9.7, it was determined that a minimum sample size of 107 participants would be sufficient to detect significant effects with a 95% confidence level (α = 0.05), a statistical power of 0.95, and a moderate effect size (f2 = 0.15), considering at least two independent variables. However, a larger sample of 404 participants was included to enhance the precision of the statistical analyses, improve representativeness, and account for potential data loss.
Ethical considerations
The study was approved by the Ethics Committee of the Universidad Peruana Unión [Approval number: 2024-CEB-FCS-UPeU-N°296], adhering to the ethical principles outlined in the Declaration of Helsinki. Participants were provided with detailed information about the research objectives, the voluntary nature of their participation, and their right to withdraw at any time without repercussions. Additionally, confidentiality and the anonymous handling of the data collected were ensured. Prior to participation, all individuals provided informed consent in digital format, which was made available through the platform used for data collection.
Variables and measuring instruments
Nutritional knowledge
The questionnaire of habits and knowledge about dietary fiber conducted by Martinho was used42. This tool was divided into five sections and assessed the respondent’s opinions on various topics. Consumption habits were evaluated on a scale from 0 to 7. Knowledge about dietary fiber, including its relationship with food varieties and diseases, was assessed using a Likert scale ranging from 1 (totally disagree) to 5 (totally agree). For food labeling, responses were rated on a scale from ‘never’ to ‘always’. The instrument was adapted to Spanish and previously validated in similar Spanish-speaking contexts43. In this study, the questionnaire demonstrated good internal consistency, with a Cronbach’s alpha of 0.789.
Fiber intake
The assessment of fiber-rich food consumption was conducted using an instrument developed by Block, designed to measure the frequency of consumption across seven food groups: cereals, vegetables, fruits, oilseeds, miscellaneous, legumes, and tubers44. Participants rated the frequency of consumption using a scale with the following response options: less than once per week (0), once per week (1), 2 to 3 times per week (3), 4 to 6 times per week (4), and every day (5). This instrument evaluated eating habits over the 12 months preceding the interview.
The questionnaire included a structured self-scoring system for interpreting the results: a score of 30 or more indicated ‘You are doing great!‘; a score between 20 and 29 suggested ‘You should include more fruits, vegetables, and whole grains’; and a score below 20 indicated ‘Your diet is probably low in important nutrients.’ You should find ways to increase the fruits, vegetables, and other fiber-rich foods you eat daily. In this study, the outcome was defined as ‘inadequate frequency of fiber-rich food intake,’ with individuals scoring below 20 being classified as positive for this condition45. In the current study, the scale achieved a McDonald’s Omega coefficient of 0.741.
BMI
Participants’ weight and height were self-reported via the virtual questionnaire, as data collection was conducted remotely. BMI was calculated using the formula weight/height2 (kg/m2) and classified according to the parameters established by the WHO46. The categories were defined as follows: underweight (BMI ≤ 18.5 kg/m2), normal weight (BMI 18.5–24.9 kg/m2), overweight (BMI 25.0–29.9 kg/m2), and obese (BMI ≥ 30 kg/m2). To enhance the accuracy of self-reported BMI, participants were instructed to provide their most recent weight and height measurements, preferably from a recent medical check-up or home scale measurement. Studies have shown that self-reported anthropometric data can be reliable in epidemiological research, particularly when participants are guided to report their most recent objective measurements47. Additionally, we conducted data screening for implausible values (e.g., extreme outliers), which were cross-checked with participants when necessary. This classification, based on WHO international guidelines, allowed for the assessment of participants’ nutritional status within a population context while adapting to the virtual data collection format48.
Symptoms of constipation
To assess the degree of symptomatology associated with functional constipation, the International Diagnostic Questionnaire for Pediatric Functional Gastrointestinal Disorders, Rome III version, was utilized. This instrument, consisting of 7 items, examines aspects such as evacuation frequency, stool consistency and volume, painful defecation, and retentive postures adopted to avoid excretion. Participants were classified as symptomatic of functional constipation if they provided at least three responses indicative of symptomatology across the seven items evaluated. The validity of the instrument was determined using Cohen’s Kappa coefficient, with values ranging from 0.4 to 0.7.
Statistical analysis
Statistical analysis was performed using R Studio (version 4.2.1) and SPSS (version 29). Descriptive analysis included the calculation of means and standard deviations for the study variables, while sociodemographic characteristics were summarized in detailed tables. The graphs were created in Python 3.9 using the Matplotlib, NumPy, and Pandas libraries in the Jupyter Notebook environment.
Inferential analysis involved the use of Pearson’s correlation coefficient and Student’s t-test to explore bivariate relationships, followed by hierarchical regression analysis to examine the explanatory contribution of each independent variable on constipation symptoms. The hierarchical regression model was chosen due to its ability to assess the incremental explanatory power of different independent variables in a sequential manner. This approach allows for a structured examination of how much variance in constipation symptoms is explained by each set of independent variables (nutritional knowledge, fiber intake, BMI, and sex), controlling for the influence of previously entered variables.
Results
The study sample comprised 404 participants with a mean age of 34.75 years (SD = 12.88). Regarding sex, 66.1% were women (n = 267). In terms of educational level, the majority (82%) reported having a university education (n = 331). Regarding marital status, 63.1% of participants were single (n = 255). In terms of geographic origin, more than half (53.5%) were from the coastal region (n = 216), followed by 31.2% from the jungle region (n = 126) (see Table 1).
Table 2 highlights significant differences in nutritional knowledge based on age (p = 0.010, CI [− 2.065, − 0.286]), suggesting that older individuals possess greater knowledge. “However, no significant differences were found in nutritional knowledge based on sex (p = 0.537), educational level (p = 0.307), or marital status (p = 0.116). Fiber-rich food consumption was significantly higher among married or cohabiting individuals (p = 0.003, CI [3.601, 17.783]) and older adults (p = 0.027, CI [− 14.423, − 0.865]), but no significant differences were observed based on sex (p = 0.085) or educational level (p = 0.710). BMI was significantly higher among men (p = 0.001, CI [0.384, 1.493]) and older individuals (p = 0.001, CI [− 1.440, − 0.362]). However, no significant differences were observed based on educational level (p = 0.871) or marital status (p = 0.251). Finally, constipation symptoms did not show significant differences based on sex (p = 0.277), educational level (p = 0.188), marital status (p = 0.056), or age (p = 0.255).
Figure 1 shows a negative and significant correlation between nutritional knowledge and constipation symptoms (r = − 0.26, p < 0.001, CI [− 0.373, − 0.132]), suggesting that higher nutritional knowledge is associated with fewer reported constipation symptoms. Similarly, a negative and significant correlation was found between high-fiber food consumption and constipation symptoms (r = − 0.29, p < 0.001, CI [− 0.404, − 0.168]), indicating that greater fiber intake is associated with a reduction in constipation symptoms. On the other hand, a positive and significant correlation was observed between BMI and constipation symptoms (r = 0.25, p < 0.001, CI [0.127, 0.368]), suggesting that a higher BMI is associated with an increase in constipation symptoms.

Correlation analysis between nutritional knowledge, frequency of fiber-rich food consumption, BMI, and constipation. NK nutritional knowledge, FI fiber intake, BMI body mass index, CS constipation symptoms. *p < 0.05; *p < 0.01; [x, x] = 95% Confidence Interval. The color intensity reflects the magnitude of the correlation: dark red indicates strong negative correlations, dark blue indicates strong positive correlations, and lighter shades represent weak or near-zero correlations. The color bar illustrates the correlation strength, where higher intensity indicates a stronger correlation, approaching 1 or − 1.
Table 3 presents the hierarchical regression analysis for constipation symptoms, demonstrating a progressive increase in the explained variance as new variables are introduced in each block. In Block 1, nutritional knowledge shows a significant negative effect on constipation symptoms (β = − 0.256, p < 0.001, CI [− 0.382, − 0.131]), indicating that higher nutritional knowledge is associated with fewer reported symptoms. This block accounts for 6.2% of the variance (adjusted R2 = 0.062). In Block 2, with the addition of fiber intake (FI) alongside nutritional knowledge (NK, both variables retain significant negative associations (NK: β = − 0.191, p = 0.003, CI [− 0.318, − 0.065]; FI: β = − 0.238, p < 0.001, CI [− 0.365, − 0.111]), suggesting that increased fiber intake is associated with a reduction in constipation symptoms. The ∆R2 = 0.052, indicating an additional 5.2% of the variance explained, bringing the total variance explained to 11.0% (adjusted R2 = 0.110). In Block 3, the inclusion of BMI reveals a significant positive association with constipation symptoms (β = 0.199, p = 0.001, CI [0.078, 0.321]), suggesting that a higher BMI increases symptom severity. Meanwhile, the other variables retain their significant negative effects (NK: β = − 0.174, p = 0.007, CI [− 0.299, − 0.049]; FI: β = − 0.214, p = 0.001, CI [− 0.339, − 0.089]). The ∆R2 = 0.039, accounting for an additional 3.9% of the variance, resulting in a total variance explained of 14.6% (adjusted R2 = 0.146). Finally, in Block 4, the inclusion of sex reveals a significant positive association with constipation symptoms (β = 0.153, p = 0.014, CI [0.031, 0.274]), indicating that being female is associated with more constipation symptoms compared to males. The other variables retain their significant effects (NK: β = − 0.173, p = 0.006, CI [− 0.296, − 0.050]; FI: β = − 0.227, p < 0.001, CI [− 0.351, − 0.103]; BMI: β = 0.230, p < 0.001, CI [0.108, 0.353]). The ∆R2 = 0.022, accounting for an additional 2.2% of the variance, bringing the total variance explained to 16.4% (adjusted R2 = 0.164). This analysis demonstrates a gradual increase in R2 with the addition of each new variable. The largest change in R2 is observed with the addition of fiber-rich food consumption in Block 2, accounting for an additional 5.2%, underscoring the critical role of dietary habits in reducing symptoms. The smallest change occurs with the inclusion of sex in Block 4, contributing only an additional 2.2%, though it remains relevant in explaining the issue. Collectively, the four variables—nutritional knowledge, high-fiber food consumption, BMI, and sex—account for 16.4% of the variability in constipation symptoms, emphasizing that both dietary habits and individual factors (BMI and sex) are crucial for understanding the manifestation of symptoms. Figure 2 illustrates both ∆R2 and adjusted R2.

Hierarchical regression model for constipation symptoms. The figure illustrates the changes in explained variance (∆R2, light blue) and adjusted R2 (dark blue) in each block of the hierarchical regression model for constipation symptoms. Each block incorporates new variables (nutritional knowledge, fiber intake, BMI, and sex), and the values within the bars represent the corresponding decimal coefficients. Higher values indicate a better model fit.
Discussion
Functional constipation is a prevalent gastrointestinal disorder that has a substantial impact on individuals’ quality of life8. Factors such as nutritional knowledge, fiber-rich food intake, BMI, and sociodemographic characteristics, including sex, have been identified in the literature as factors associated with this condition6,13,26,33,37, although their interactions remain a topic of debate. This study sought to address these relationships in a Peruvian context, providing evidence on the importance of the aforementioned factors in the prevalence and severity of constipation symptoms. The main findings of the study were as follows: (a) nutritional knowledge was significantly associated with a reduction in constipation symptoms; (b) similarly, higher fiber consumption was linked to a decrease in symptoms; (c) conversely, higher BMI and being female were associated with an increase in constipation symptoms; and (d) collectively, the analyzed variables explained 16.4% of the total variance in symptoms (adjusted R2 = 0.164), with fiber-rich food consumption emerging as one of the most influential variables, contributing an additional 5.2% to the explained variance (∆R2 = 0.052).
Nutritional knowledge
Nutritional knowledge plays an important role in promoting healthy eating habits and preventing gastrointestinal disorders such as constipation10. In our study, increased nutritional knowledge was found to be significantly associated with a reduction in constipation symptoms, which is consistent with previous findings highlighting the positive influence of knowledge on the adoption of a healthy diet, which is important for improving digestive health11,12.
This finding may be explained by the fact that people with greater nutritional knowledge tend to be better informed about the importance of consuming fiber-rich foods and other healthy habits, such as increased water intake, which are fundamental to preventing constipation13. Similar have shown that educational interventions aimed at increasing nutritional knowledge can significantly improve the consumption of fiber-rich foods, such as fruits, vegetables, and whole grains. This, in turn, improves intestinal motility and stool consistency17,18,19. These findings underscore the importance of implementing nutrition education programs as a preventive measure in populations with a high prevalence of constipation, especially in contexts where dietary habits do not align with international recommendations.
Fiber intake
It is important to note that an inadequate diet, especially a low fiber intake, is one of the main factors associated with constipation7. Dietary fiber contributes to the bulk and consistency of the stool, facilitating its transit through the intestinal tract26. In this regard, a diet lacking in fruits, vegetables, legumes, and whole grains has been identified as a significant risk factor for the development of constipation7. The current study found that higher consumption of fiber-rich foods was associated with a significant decrease in constipation symptoms. This supports existing evidence for the benefits of dietary fiber on gastrointestinal health. For instance, in the national context, studies have identified a statistical relationship between fiber intake and constipation27,28. Similarly, Yang et al.26, also support this claim in a meta-analysis, which suggests that low fiber intake is one of the most prevalent factors of constipation. Additionally, previous studies indicate that fiber supplementation can contribute to reducing the duration of constipation episodes21,25. In fact, soluble fiber supplements with high viscosity and low fermentation, such as psyllium and konjac glucomannan, have been shown to effectively soften stools, facilitate evacuation, and relieve symptoms of constipation, offering a therapeutic option in cases of functional constipation49.
In addition, it has been suggested that fiber intake may significantly affect intestinal transit time, especially in individuals with prolonged initial transit (> 48 h)50. In this group, the transit time was reduced by approximately 30 min for each additional gram of fiber from grains, fruits, or vegetables, regardless of whether the fiber was fermentable or not49,51. However, in individuals with a shorter initial transit time (< 48 h), increased fiber intake does not appear to produce a significant change in this parameter49. The mechanisms that explain this relationship include not only the physical effects of fiber in the colon, but also its ability to ferment and produce short-chain fatty acids that stimulate bowel motility and improve the gut microbiome52. These findings underscore the importance of including fiber-rich foods such as fruits, vegetables, whole grains, and legumes in the daily diet as an effective preventive and therapeutic strategy for constipation.
Elevated BMI
Another important finding of the current study is that a higher BMI is associated with an increase in constipation symptoms, highlighting the complex relationship between nutritional status and gastrointestinal health. This finding is consistent with previous research that has reported a higher prevalence of constipation in overweight or obese individuals, considering various indicators of obesity such as BMI, waist to height ratio (WSR), lipid accumulation products (LAP), and weight adjusted waist index (WWI)6,33. For example, a recent study found a significant non-linear relationship between BMI, WSR, and LAP in relation to constipation, suggesting that an increase in these obesity indices is associated with an increased risk of constipation33. In addition, a study analyzing baseline data from a randomized clinical trial of Brazilian adults aged 18 to 64 years found a high prevalence of constipation in adults with class II and III obesity6.
Obesity may contribute to constipation through several interrelated mechanisms. On the one hand, obesity is often associated with a sedentary lifestyle and low dietary quality, characterized by low fiber and vegetable intake in general, which reduces bowel motility and predisposes to the development of functional constipation31. On the other hand, it has been proposed that obesity indirectly affects bowel habits by altering gut hormone secretion and impairing gut motility, key factors in gastrointestinal transit33. Chronic low-grade inflammation associated with obesity also plays an important role, as it can affect neurogastrointestinal regulation and colonic muscle function, exacerbating constipation symptoms32. Similarly, the accumulation of adipose tissue, especially in the abdominal region, could put mechanical pressure on the digestive organs and alter intestinal transit53. However, studies in other populations have found conflicting results, revealing a non-linear association between WWI and chronic constipation; a low WWI (i.e., below the inflection point of 9.77) was associated with an increased risk of chronic constipation, suggesting that factors such as sex, diet, and physical activity may modulate this relationship35. Therefore, it is important to address overweightness and obesity not only from a metabolic perspective, but also to consider its impact on digestive health to develop comprehensive strategies to prevent and alleviate constipation in people with a high BMI.
Sex
On the other hand, being female is associated with an increase in constipation symptoms. Similarly, previous research has documented a higher prevalence of this disorder in women compared to men36,38,39. This finding may be explained by a combination of biological, hormonal, and social factors. Biologically, differences in pelvic anatomy and pelvic floor function may predispose women to reduced bowel motility and defecation difficulties37. At a hormonal level, fluctuations in estrogen and progesterone levels, particularly during the menstrual cycle, pregnancy, and menopause, can slow gastrointestinal motility and reduce the rate of intestinal transit54. Additionally, beyond its effects on motility, hormonal fluctuations may also influence gut microbiota composition and visceral sensitivity, mechanisms that have been proposed as additional contributors to sex differences in functional constipation55. On the other hand, psychosocial factors play an important role. Women are more likely to report symptoms of constipation, possibly due to greater awareness and self-perception of digestive issues, as well as differences in medical consultation behaviors compared to men37,54. Dietary and lifestyle factors also contribute to this disparity, as women often have lower overall energy intake, differences in macronutrient composition, and variations in hydration habits, which can influence bowel function56.
Given these findings, it is crucial to develop gender-sensitive interventions for the prevention and management of constipation. Public health strategies should include targeted education on the impact of hormonal changes on digestive health, emphasize the importance of adequate fiber and water intake in women, and promote pelvic floor exercises to support bowel motility. Additionally, raising awareness among healthcare professionals about gender-specific patterns in constipation prevalence may enhance diagnosis and treatment approaches.
Total variance in constipation symptoms
The finding that the variables analyzed explained 16.4% of the total variance of constipation symptoms (adjusted R2 = 0.164) highlights the importance of addressing this disorder from a multifactorial approach. Among these variables, the consumption of fiber-rich foods stood out as one of the most influential, contributing a 5.2% increase in the variance explained (∆R2 = 0.052). This finding is consistent with previous research highlighting the central role of fiber in preventing constipation symptoms1,20,25,49. The relatively high contribution of dietary fiber intake to the model suggests that this factor has a tangible and direct impact on constipation symptoms, reinforcing the need to promote educational and dietary strategies to increase its intake in the general population. Although the percentage of variance explained by the model is moderate, it reflects the complexity of constipation, a condition likely influenced by an interaction of biological, behavioral, and environmental factors that requires a comprehensive approach for its effective management.
Public health implications
The results of this study highlight important public health implications for the prevention and management of functional constipation in the general population. One of the priorities identified is the promotion of high-fiber diets as an accessible and cost-effective strategy to improve digestive health. Public health initiatives should focus on increasing awareness of the benefits of fiber through educational campaigns and the integration of nutrition education into community programs, especially in populations where fiber intake is inadequate. These actions would not only help reduce dietary deficiencies, but also promote sustainable changes in dietary habits.
In addition, the results of the study underscore the need to implement educational programs that improve knowledge about the importance of a diet rich in fiber and its impact on gut health. These campaigns should target different population groups, with content adapted to their level of understanding and cultural context. This inclusive approach could become an effective tool to promote sustainable changes in dietary habits, thereby reinforcing the positive impact of public health policies in preventing constipation and improving the quality of life of the population.
On the other hand, it highlights the need to address obesity as a multifactorial health challenge. Interventions aimed at weight management through dietary modification, promotion of physical activity, and behavioral support could not only reduce the prevalence of obesity, but also alleviate the associated gastrointestinal symptoms. Given the complexity of obesity-related constipation, it is essential to implement tailored approaches that consider the individual characteristics and socioeconomic contexts of those affected. Furthermore, this study highlights the disproportionate burden of constipation in women, suggesting the need for sex-specific interventions. Public health programs should prioritize research and resource allocation to understand and address the hormonal, biological, and psychosocial factors that contribute to constipation in women. This includes considering sex differences in symptom patterns and their impact on quality of life when designing prevention and treatment strategies.
Limitations and future research
This study has several limitations that should be considered when interpreting the results. First, due to the cross-sectional design of the research, it is not possible to establish causal relationships between the variables analyzed and constipation symptoms. Future research could use longitudinal or experimental designs to assess how changes in dietary knowledge, fiber intake, and BMI affect the development and management of constipation over time. Second, data collection was remote and self-reported, which may introduce response bias, especially for anthropometric variables such as weight and height. Although this method allowed information to be collected from a large and diverse sample, it is recommended that future studies be supplemented with objective measurements performed by health professionals to increase the accuracy of the data.
Another limitation of this study is the use of non-probabilistic purposive sampling, which may limit the generalizability of the results to the broader Peruvian population. Since the sample was not randomly selected, certain socio-demographic groups may be overrepresented or underrepresented, potentially influencing the findings. Future studies should consider sampling methods that ensure greater representativeness of the Peruvian population in terms of socio-demographic and geographic characteristics.
Another limitation of the current study is the lack of evaluation of water intake, which plays a critical role in the effectiveness of dietary fiber in preventing and managing constipation. Adequate hydration is essential for fiber to increase stool bulk and promote bowel motility; thus, variations in water intake among participants could have influenced the observed associations. Future research should incorporate comprehensive dietary assessments that include fluid intake alongside fiber consumption to provide a more complete understanding of their combined effects on constipation symptoms.
Additionally, our study did not differentiate between types of dietary fiber (soluble vs. insoluble) or the precise amounts consumed, which could have influenced the results. While the instrument used provided an overall measure of fiber-rich food consumption, different fiber sources have distinct physiological effects on bowel function. Future studies should aim to quantify specific fiber intake and its interaction with other dietary factors to refine the understanding of its role in constipation management.
Finally, although the model explained 16.4% of the variance in constipation symptoms, this suggests that there are other relevant factors that were not considered in this study, such as psychosocial, genetic, or gut microbiome-related aspects. Future research could explore these additional variables to provide a more comprehensive view of the factors contributing to functional constipation. We would like to make it clear that these limitations do not diminish the relevance of the study findings, but rather open up important opportunities for future research to further explore this area.
Conclusion
The results confirmed that greater nutritional knowledge and higher fiber intake were associated with a reduction in symptoms, while high BMI and being female were associated with an increase in symptoms. These variables together explained 16.4% of the total variance in symptoms, highlighting the importance of fiber intake as one of the most influential factors. These findings underscore the need for targeted educational interventions to improve nutrition knowledge and promote healthy eating habits, as well as strategies to address the impact of increased BMI and sex differences in the management of constipation. Therefore, healthcare professionals should integrate dietary counseling focused on fiber intake into routine consultations, emphasizing its role in digestive health. Policymakers should prioritize the development and implementation of nutrition education programs at the community level, particularly for high-risk groups such as individuals with obesity and women.
Data availability
The data sets generated to support the findings of this study are not publicly available, but can be requested from the corresponding author.
References
Sayuk, G. S., Yu, Q. T. & Shy, C. Management of constipation in hospitalized patients. J. Clin. Med. 12, 6148 (2023).
Forootan, M., Bagheri, N. & Darvishi, M. Chronic constipation. Medicine 97, e10631 (2018).
Sanchez, M. I. P. & Bercik, P. Epidemiology and burden of chronic constipation. Can. J. Gastroenterol. 25, 11B–15B (2011).
Pontet, Y. & Olano, C. Prevalencia de síndrome de intestino irritable En América Latina. Revista De Gastroenterología Del. Perú. 41, 144 (2021).
Arellano, C. Estreñimiento Crónico Funcional En Estudiantes De 7 Años De Edad Por El Bajo Consumo De Fibra Y Liquidos En Su Dieta Diaria (Universidad San Ignacio de Loyola, 2020).
Silveira, E. A. et al. e Prevalence of constipation in adults with obesity class II and III and associated factors. BMC Gastroenterol ; 21: 217. (2021).
Rollet, M., Bohn, T. & Vahid, F. Association between dietary factors and constipation in adults living in Luxembourg and taking part in the ORISCAV-LUX 2 survey. Nutrients 14, 122 (2021).
Lin, J-N. et al. Living with constipation and communication taboos surrounding constipation among older adults: an interpretive phenomenology analysis study. Geriatr. Nurs. (Minneap). 58, 266–273 (2024).
Albu, A. et al. The economic burden of constipation therapy. Med Pharm Rep. Epub ahead of print 23 May 2019. https://doi.org/10.15386/mpr-1222
Cusquisibán-Alcantara, Y. et al. Impact of a nutrition education intervention on knowledge, healthy eating index, and biochemical profile in a rural community in Peru. J. Multidiscip Healthc. 17, 1111–1125 (2024).
Thomas, A., Thomas, A. & Butler-Sanchez, M. Dietary modification for the restoration of gut Microbiome and management of symptoms in irritable bowel syndrome. Am. J. Lifestyle Med. 16, 608–621 (2022).
Silva, P. et al. Nutrition and food literacy: framing the challenges to health communication. Nutrients 15, 4708 (2023).
Alfawaz, H. et al. Awareness and knowledge regarding the consumption of dietary fiber and its relation to Self-Reported health status in an adult Arab population: A Cross-Sectional study. Int. J. Environ. Res. Public. Health. 17, 4226 (2020).
Mandeville, K. L. et al. Gastroenterology in developing countries: issues and advances. World J. Gastroenterol. 15, 2839 (2009).
Dovey, T. M., Sinopoulou, V. & Gordon, M. Psychological and educational interventions for childhood constipation. Cochrane Database of Systematic Reviews; Epub ahead of print 6 July 2023. (2023). https://doi.org/10.1002/14651858.CD014578
Yildirim, A. et al. The effect of education given to children with functional constipation and fecal incontinence and their mothers on anxiety and constipation management. Florence Nightingale J. Nurs. 28, 321–332 (2020).
Ho, K-S. Stopping or reducing dietary fiber intake reduces constipation and its associated symptoms. World J. Gastroenterol. 18, 4593 (2012).
Bellini, M. et al. Low FODMAP diet: evidence, doubts, and hopes. Nutrients 12, 148 (2020).
Dionne, J. et al. A systematic review and Meta-Analysis evaluating the efficacy of a Gluten-Free diet and a low FODMAPS diet in treating symptoms of irritable bowel syndrome. Am. J. Gastroenterol. 113, 1290–1300 (2018).
Shen, L. et al. Lower dietary fibre intake, but not total water consumption, is associated with constipation: a population-based analysis. J. Hum. Nutr. Dietetics. 32, 422–431 (2019).
van der Schoot, A. et al. The effect of fiber supplementation on chronic constipation in adults: an updated systematic review and Meta-Analysis of randomized controlled trials. Am. J. Clin. Nutr. 116, 953–969 (2022).
Ioniță-Mîndrican, C-B. et al. Therapeutic benefits and dietary restrictions of fiber intake: A state of the Art review. Nutrients 14, 2641 (2022).
Outcome of the Public consultation on the Draft Opinion of the Scientific Panel on Dietetic. products, Nutrition, and Allergies (NDA) on Dietary Reference Values for carbohydrates and dietary fibre. EFSA Journal; 8. Epub ahead of print March 2010. https://doi.org/10.2903/j.efsa.2010.1508
INEI. Gobierno del Perú. Solo el 11.3% de la población peruana mayor de 15 años consume la cantidad de frutas y verduras que recomienda la OMS & Lima Perú, (2020). https://web.ins.gob.pe/index.php/es/prensa/noticia/ (accessed 5 January 2021).
McRae, M. P. Effectiveness of fiber supplementation for constipation, weight loss, and supporting Gastrointestinal function: A narrative review of Meta-Analyses. J. Chiropr. Med. 19, 58–64 (2020).
Yang, J. Effect of dietary fiber on constipation: A meta analysis. World J. Gastroenterol. 18, 7378 (2012).
Mauricio, J. Relación entre el consumo de fibra y la presencia de estreñimiento en niños atendidos en el Centro De Salud Virgen Del Carmen - La Era, Lima 2015. Universidad Peruana Unión, (2015).
Vilchez, J. Consumo De Fibra Dietaria, De Alimentos Ultraprocesados Y Estreñimiento En Pacientes Operados De Apendicitis En Hospital Nacional, Jaen 2022 (Segunda Especialidad, Universidad Nacional Mayor de San Marcos,, 2023).
PAHO/WHO. Obesity Prevention - PAHO/WHO | Pan American Health Organization, (2021). https://www.paho.org/en/topics/obesity-prevention (Accessed 9 May 2023).
INEI. Perú: Enfermedades No Transmisibles Y Transmisibles, 2023 (Lima, 2024).
Alsheridah, N. & Akhtar, S. Diet, obesity and colorectal carcinoma risk: results from a National cancer registry-based middle-eastern study. BMC Cancer. 18, 1227 (2018).
Corsello, A. et al. Gut dysmotility in children with neurological impairment: the nutritional management. Front Neurol; 14. Epub ahead of print 5 May 2023. https://doi.org/10.3389/fneur.2023.1200101
Xiang, N. et al. Multiple obesity indices suggest a close relationship between obesity and constipation: evidence from NHANES. BMC Public. Health. 24, 1273 (2024).
Ogasawara, N. et al. Relationships between body mass index and constipation, gastroesophageal reflux disease, stool forms based on the Bristol stool form scale, and education level: results from an internet survey in Japan. J. Clin. Biochem. Nutr. 73, 22–143 (2023).
Yang, X. & Sun, Z. Association between weight-adjusted-waist index and bowel habits. Sci. Rep. 14, 17658 (2024).
Verkuijl, S. J. et al. The influence of demographic characteristics on constipation symptoms: a detailed overview. BMC Gastroenterol. 20, 168 (2020).
Almeida Gomes Dantas, A. et al. Is constipation associated with worse functioning in adult women?? A Cross-Sectional study. J. Multidiscip Healthc. ; 13: 883–889. (2020).<\/p>
Schmidt, F. M. Q., Santos, V. L. C. & de Domansky, G. Prevalence of self-reported constipation in adults from the general population. Revista Da Escola De Enfermagem Da USP. 49, 440–449 (2015).
Tamura, A. et al. Prevalence and Self-recognition of chronic constipation: results of an internet survey. J. Neurogastroenterol Motil. 22, 677–685 (2016).
Collete, V. L., Araújo, C. L. & Madruga, S. W. Prevalência e fatores associados à Constipação intestinal: Um Estudo de base populacional Em Pelotas, Rio Grande do Sul, Brasil, 2007. Cad Saude Publica. 26, 1391–1402 (2010).
Ato, M., López, J. J. & Benavente, A. Un sistema de Clasificación de Los Diseños de investigación En psicología [A classification system of research designs in psychology]. Anales De Psicología. 29, 1038–1059 (2013).
Costa Martinho, C. A. Estudo Sobre O Conhecimento Da População Portuguesa Acerca De Fibras Alimentares (Instituto Politécnico de Viseu, 2011).
Dundur, N. Conocimiento sobre los beneficios del consumo de fibra dietética en Santa Cruz, Bolivia y propuesta de un chocolate funcional. Tesis de Licenciatura, Universidad Zamorano, (2021).
Thompson, F. E. & Byers, T. Dietary assessment resource manual. J. Nutr. 2297S–2298S. (1994).
Madruga, S. W., Araújo, C. L. & Bertoldi, A. D. Frequency of fiber-rich food intake and associated factors in a Southern Brazilian population. Cad Saude Publica. 25, 2249–2259 (2009).
. Gobierno del Perú. Guía técnica para la valoración nutricional antropométrica de la persona adulta, (2012). https://repositorio.ins.gob.pe/xmlui/handle/INS/225 accessed 24 June 2020).
Davies, A. et al. Validity of self-reported weight and height for BMI classification: A cross-sectional study among young adults. Nutrition 71, 110622 (2020).
Fayyaz, K. et al. Validity of measured vs. Self-Reported weight and height and practical considerations for enhancing reliability in clinical and epidemiological studies: A systematic review. Nutrients 16, 1704 (2024).
Dreher, M. L. Fiber in laxation and constipation. In: Dietary Fiber in Health and Disease. Cham: Springer International Publishing, 95–115. (2018).
de Vries, J. Effects of cereal fiber on bowel function: A systematic review of intervention trials. World J. Gastroenterol. 21, 8952 (2015).
De Vries, J. et al. Effects of cereal, fruit and vegetable fibers on human fecal weight and transit time: A comprehensive review of intervention trials. Nutrients 8, 130 (2016).
Xu, X. et al. Chronic constipation and gut microbiota: current research insights and therapeutic implications. Postgrad. Med. J. 100, 890–897 (2024).
Miron, I. Gastrointestinal motility disorders in obesity. Acta Endocrinol. (Bucharest). 15, 497–504 (2019).
Dantas, A. A. G. et al. Prevalence and factors associated with constipation in premenopausal women: a community-based study. Arq. Gastroenterol. 57, 188–192 (2020).
Marano, G. et al. Irritable bowel syndrome: A hallmark of psychological distress in women?? Life 15, 277 (2025).
Warren, A. The relationship between gender differences in dietary habits, neuroinflammation, and Alzheimer’s disease. Front Aging Neurosci; 16. Epub ahead of print 17 April 2024. https://doi.org/10.3389/fnagi.2024.1395825
Acknowledgements
The authors would like to thank the Universidad Peruana Unión for its institutional support of this study. We would also like to thank all of the participants who volunteered their time and effort to fill out the questionnaires, making it possible to collect the necessary data. Finally, we extend our appreciation to the colleagues and professionals who offered valuable suggestions and guidance during the development of this work.
Funding
The research was carried out with the funding of the researchers.
Author information
Authors and Affiliations
Contributions
PCR-R: Conceptualization of the study, methodological design, and drafting of the manuscript. DJ-A: Data collection, statistical processing, critical revision of the manuscript, and final editing. YEC-M: Data collection, and contribution to the writing of the results section, critical revision of the manuscript and final editing. JS: Academic supervision, critical revision of the manuscript, conceptual input into the theoretical framework and discussion, and final editing. All authors reviewed and approved the final version of the manuscript for publication.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
The study was approved by the Ethics Committee of the Universidad Peruana Unión [Approval number: 2024-CEB-FCS-UPeU-N°296], adhering to the ethical principles outlined in the Declaration of Helsinki. Participants were provided with detailed information about the research objectives, the voluntary nature of their participation, and their right to withdraw at any time without repercussions. Additionally, confidentiality and the anonymous handling of the data collected were ensured. Prior to participation, all participants were provided written informed consent.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Rojas-Rojales, P.C., Javier-Aliaga, D., Calizaya-Milla, Y.E. et al. Nutritional knowledge, fiber intake, body mass index, and sex associated with constipation symptoms in Peruvian adults. Sci Rep 15, 12673 (2025). https://doi.org/10.1038/s41598-025-97671-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-025-97671-3
